SEARCH RESULTS FOR: Cirrhosis
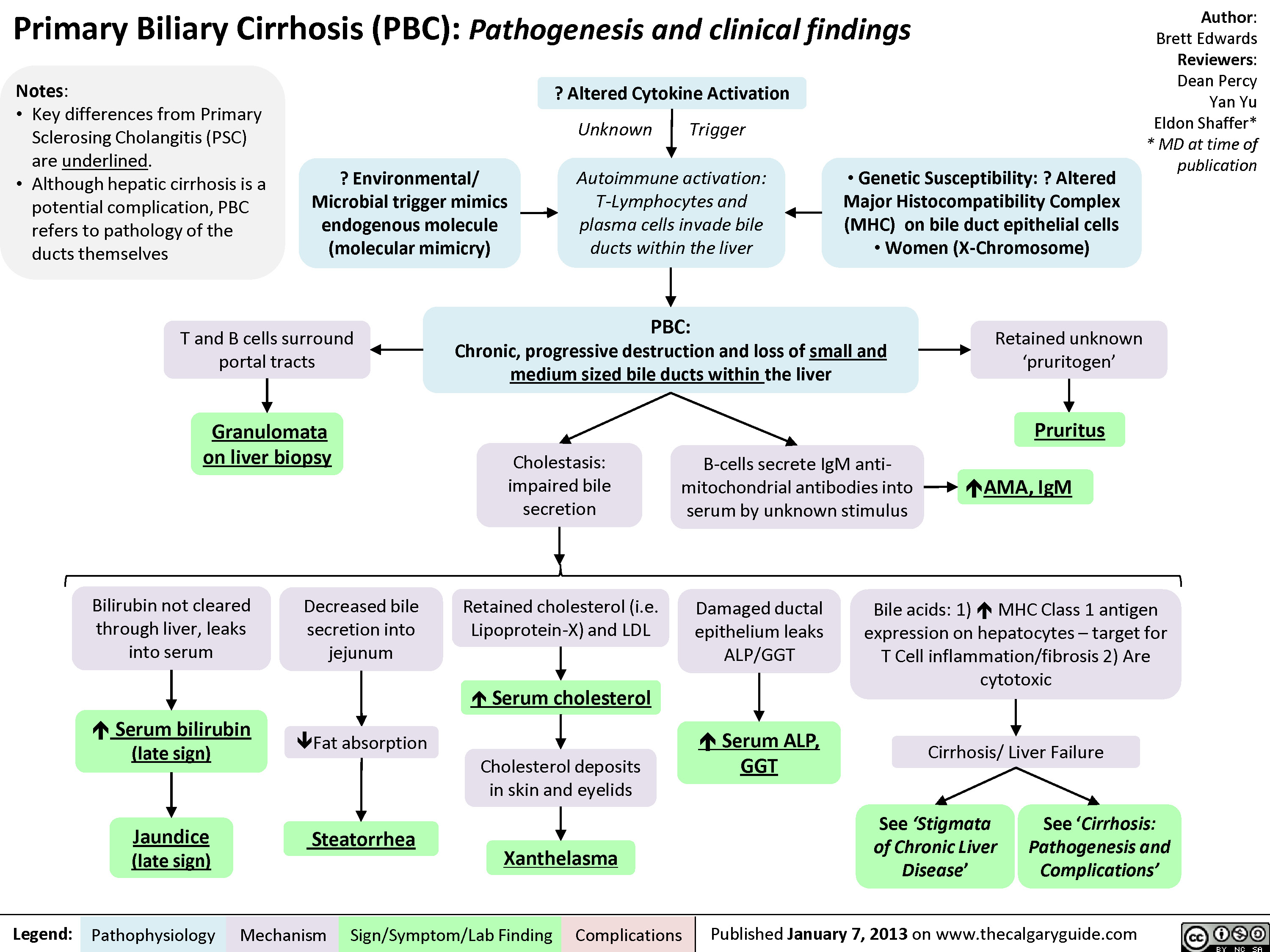
Primary Biliary Cirrhosis (PBC)
esophageal-gastric-varices

Legend:
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
• Venous drainage of spleen backed up into gastric anastomoses
Tachycardia and hypotension
Anemia Death Melena Coffee ground emesis Hematemesis Bright red blood per rectum")
Hepatitis C (HCV) Infections: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Hepatitis C (HCV) Infection: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Biliary Atresia (BA)- Pathogenesis and clinical findings
- Pathogenesis and clinical findings Intrauterine environment genetic factors abnormal bile duct development toxic inflammatory response viral immunologic injury to bile duct epithelia pathophysiology poorly understood histology consistent with obstruction on liver biopsy biliary atresia progressive idiopathic fibre-obliterative disease extra-hepatic biliary tree biliary obstruction on intra-operative cholangiogram (diagnostic) partial complete bile duct obstruction delivery of bile acids to small intestine pressure in bile duct absorption of fat and soluble vitamins vitamin K+ deficiency coagulopathy INR PTT bruising petechiae acholic pale stool failure to thrive elimination of bilirubin conjugated direct bilirubin jaundice pruritus excreted urine dark urine diaper yellow pressure bile duct GGT backs up in liver cholestatic hepatitis firm enlarged liver fibrosis cirrhosis ALT AST Horwitz Adderley McKenzie")
Wilson's Disease

Hepatic Cu accumulation, deposition in hepatocyte lysosomes
Hepatocyte injury (speculated mechanism: free radicals)
Cu leak from damaged hepatocytes
Epidemiology:
• Autosomal Recessive condition with prevalence of 1:30,000 • 60% of cases present initially with neurologic Symptoms
• Fulminant cases present with acute liver failure and massive
hemolysis, treated with liver transplant
↓ ceruloplasmin release ↓ serum ceruloplasmin
Early asymptomatic liver dysfunction
Cu movement into bloodstream
Cu deposition in vulnerable tissues
Abbreviations:
• Cu - Copper
• AST - Aspartate Aminotransferase • ALT - Alanine Aminotransferase
↑ AST, ALT, and Bilirubin
↑ Serum free Cu (total usually low due to low ceruloplasmin)
Eyes: Kayser-Fleischer rings
CNS: Neurologic disease, Psychiatric disease MSK: Arthropathies
Kidney: Fanconi syndrome, Kidney stones
Chronic hepatitis, Cirrhosis with hepatic insufficiency, Portal hypertension, Hemolysis, Acute Liver Failure
Continued hepatocyte injuryà progressive liver damage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 17, 2019 on www.thecalgaryguide.com")
Non-Alcoholic Fatty Liver Disease
)
Steatohepatitis: chronic inflammatory and apoptotic climate in the hepatocytes (in the absence of alcohol consumption, termed Non-Alcoholic Steatohepatitis (NASH))
Fibrosis of the Liver: excessive scarring of liver tissue resulting from chronic inflammation, although liver architecture is largely intact
Fat droplets form and grow in the hepatocytes
Hepatic mitochondria increase their workload in attempt to break down the excess free fatty acids through beta-oxidation
↑ in cellular workload creates more reactive oxygen speciesà Inflammation and apoptosis of hepatocytes
On-going inflammation damages hepatic stellate cells (the primary extracellular matrix–producing cells of the liver) causing the release of fibrinogenic cytokines
Cirrhosis of the liver: normal lobular structure distorts and is replaced by regenerating nodules and bridging septa, disrupting normal liver blood flow
Deposition of fibrotic
material and collagen within the perisinusoidal spaces of the liver
Decompensated Cirrhosis Hepatocellular carcinoma
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com")
Underfill Edema Pathogenesis

Vasodilatory medications
Various mechanisms
Right-sided heart failure
Compromised right heart function ↓ forward flow
↓ Hepatic albumin synthesis
Blood is unable to pass through hepatic vessels disrupted by cirrhosis and backs up in portal vein
↑ Blood pressure in portal vein (portal hypertension)
Less blood volume in hepatic veins and vena cava (underfilling)
Pregnancy
↑ Estrogen, progesterone and relaxin
Vasodilation
Gravity causes fluid accumulation in peripheral veins
↑ Capillary hydrostatic pressure
↑ Net fluid movement into interstitial space
↓ Serum albumin
↓ Capillary oncotic pressure
Fluid extravasation into interstitial space
More blood in portal vein ↑ capillary hydrostatic pressure in venous system
Pressure creates net fluid
movement from vascular space into interstitial space
Less blood volume in arteries (underfilling)
↓ Effective arterial blood volume (EABV)
↓ Renal blood flow activates the renin-angiotensin-aldosterone system (RAAS)
Angiotensin and aldosterone ↑ Anti-diuretic hormone released by tubular Na+ and H2O resorption posterior pituitary ↑ H2O resorption
↑ Fluid in circulation, worsening existing venous congestion
↑ Hydrostatic capillary pressure and fluid extravasation into interstitial space Underfill edema (edema worsened by activation of RAAS)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 19, 2015; updated Aug 5, 2024 on www.thecalgaryguide.com")
Cystic Fibrosis

Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (transmembrane chloride ion
channel found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Pancreatic Manifestations
Trapped digestive
enzymes degrade
pancreatic tissue
Pancreatic tissue
damage triggers
inflammation,
scarring & fatty
tissue replacement
Islet cell damage
& destruction
Cystic-fibrosis related
diabetes (CFRD)
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
↓ Production & secretion of
pancreatic enzymes into GI
tract (pancreatic insufficiency)
Fat & protein malabsorption
Failure to
thrive
↓ Absorption of
fat-soluble vitamins
Steatorrhea
(↑ fat in stool)
Vitamin D
deficiency
Vitamin K
deficiency**
Rickets**
Osteoporosis**
Coagulopathies
Hepatic Manifestations
Delayed passage of bile
through biliary tree
↑ Loss of bile acids in stool
Inflammatory hepatic
response
↑ Production of lithogenic bile (bile
supersaturated with cholesterol)
Biliary cirrhosis with
portal hypertension
Cholelithiasis**
Gastrointestinal (GI) Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
**See corresponding Calgary Guide slide
Legend: Sign/Symptom/Lab Finding Complications
Pathophysiology Mechanism
Published Jan 21, 2013; updated Aug 20, 2025 on www.thecalgaryguide.com
Reproductive Manifestations
Degeneration of Wolffian duct derivatives
(vas deferens, epididymis, & seminal vesicles)
Inhibition of sperm transport
(obstructive azoospermia)
Male
infertility
Cystic Fibrosis (CF): Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Authors:
Navdeep Goraya, Spencer Montgomery
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Danielle Nelson*
*MD at time of publication
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Upper Respiratory Tract Manifestations
Retained secretions
in sinuses
Failure to clear
bacteria in sinuses
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Nasal
polyps
Chronic
sinusitis
Lower Respiratory Tract Manifestations
Retained secretions
in airways
Bacterial proliferation
in lower airway
Airway infection
& inflammation
Chronic
productive cough
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Pancreatic Manifestations
Pancreas unable to
secrete digestive enzymes
into GI tract (pancreatic
insufficiency)
Fat & protein
malabsorption
↓ Absorption of
fat-soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage
triggers inflammation,
scarring & fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
Hepatic Manifestations
Delayed passage of bile
through biliary tree
Inflammatory hepatic
response
Cirrhosis** & portal
hypertension
Gastrointestinal Manifestations
↓ Movement of
intestinal contents
In newborns:
Meconium ileus
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged jaundice
in neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
**See corresponding Calgary Guide slide
Published January 21, 2013 on www.thecalgaryguide.com
Please only review slide 1 – slides 3-7 are previous draft
versions.
Thank you!
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
Trapped digestive
enzymes degrade
pancreatic tissue
Tissue damage triggers
inflammation, scarring
& fatty tissue
replacement
Islet cell
destruction
Cystic-fibrosis related
diabetes (CFRD)
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson, Emily J. Doucette,
Mark Montgomery*, Name Name*
*MD at time of publication
In the vas deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Secretions accumulate in secretory
passages throughout the body
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Retained
secretions
in sinuses
Failure to clear
bacteria in
airways
Persistent neutrophilic inflammation triggers
tissue remodeling & mucosal overgrowth
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease (lung hyperinflation
on x-ray & abnormal pulmonary function tests)
Bronchitis ±
bronchiectasis**
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus**
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat & protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓ Serum Vitamin D
Osteoporosis**
In biliary tree
Delayed
passage of bile
Inflammatory hepatic
response
Cirrhosis** &
portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas deferens
in utero
Retained secretions
in sinuses
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion
channel that is found in exocrine tissue) dysfunction
Mutated CFTR
proteins prevent
Cl- reabsorption
in sweat glands
↑ Secretion of
Cl- into sweat
↑ Sweat Cl-
concentration
Mutated CFTR proteins in duct epithelial
tissue of other parts of the body prevent
diffusion of Cl- into secretions
↓ Cl- diffusion into peri-ciliary fluid
↓ Water composition of peri-ciliary fluid
↓ Clearance of
mucociliary secretions
Accumulation of secretions in
secretory passages throughout the
body obstructing these passages
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Degeneration of vas deferens, Wolffian
ducts & associated structures
Infertility in
affected males
In upper
respiratory
tract
Failure to clear
bacteria in
airways
Bacterial
proliferation
Chronic
sinusitis
Nasal polyps
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Airway
infection &
inflammation
Signs of obstructive lung disease i.e. lung
hyperinflation on x-ray & abnormal pulmonary
function tests
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓ Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓ Movement
of intestinal
contents
In children/adults: Distal ileal
obstruction syndrome (DIOS)
In newborns:
Meconium
ileus
↑ Retention
of meconium
↑ Reabsorption
of bilirubin
Prolonged
jaundice in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Cystic Fibrosis Transmembrane Regulator (CFTR) autosomal recessive gene mutation on chromosome 7
CFTR protein (a transmembrane chloride ion channel that is found in
exocrine tissue) dysfunction
Chloride channel no longer allows Cl- transport
CFTR proteins in
sweat glands reabsorb
Cl-
CFTR proteins in duct epithelial tissue of
other parts of the body facilitate diffusion
of Cl- into secretions
↓Reabsorption
↓Cl- diffusion into peri-ciliary fluid
↓Water composition of peri-ciliary fluid
↑Secretion of Cl-
into sweat
↓Clearance of mucociliary secretions
↑Sweat Cl-
concentration
Accumulation of secretions in secretory
passages throughout the body obstructing
these passages
Degeneration of vas deferens, Wolffian
ducts & associated structures
Authors:
Spencer Montgomery, Navdeep Goraya
Reviewers:
Yan Yu, Kayla Nelson,
Emily J. Doucette, Mark Montgomery*
*MD at time of publication
Infertility in
affected males
In upper
respiratory
tract
Retained secretions
in sinuses
Nasal polyps
Bacterial
proliferation
Chronic
sinusitis
In lower
respiratory
tract
Chronic
productive
cough
Retained
secretions in
airways
Bacterial
proliferation
Signs of obstructive lung disease
i.e. lung hyperinflation on x-ray &
abnormal pulmonary function
tests
Airway
infection &
inflammation
Bronchitis ±
bronchiectasis
Trapped digestive
enzymes degrade
pancreatic tissue
Inflammation
Scarring & fatty
tissue infiltration
Islet cell
destruction
Type II Diabetes
Mellitus
In pancreas
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and protein
malabsorption
↓Absorption of fat-
soluble vitamins
Failure to
thrive
↓Serum Vitamin D
Osteoporosis
In biliary tree
Delayed
passage
of bile
Inflammatory hepatic
response
Cirrhosis & portal
hypertension
In GI tract
↓Movement
of intestinal
contents
In children/adults: Distal ileal obstruction
syndrome (DIOS)
In
newborns:
Meconium
ileus
↑Retention
of meconium
↑Reabsorption
of bilirubin
Prolonged
jaundice
in
neonates
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published January 21, 2013 on www.thecalgaryguide.com
In the vas
deferens
in utero
Degeneration of
vas deferens,
Wolffian ducts
and associated
structures
Infertility in
affected males
Legend: Cystic Fibrosis: Pathogenesis, clinical findings, and complications
Mutation of Cystic Fibrosis Transmembrane Regulator (CFTR) gene on chromosome 7 à
Dysfunction of the CFTR protein (a transmembrane chloride ion channel that is found in exocrine tissue)
Author: Spencer Montgomery
Reviewers: Yan Yu, Kayla
Nelson, Mark Montgomery*
* MD at time of publication
Chloride channel no longer allows Cl- transport
In sweat glands, CFTR
proteins are
responsible for the
reabsorption of Cl-
In duct epithelial tissue of other parts of
the body, CFTR proteins facilitate diffusion
of Cl- into secretions
Notes:
• The CFTR mutation exhibits an autosomal recessive inheritance pattern
• > 1700 different CFTR gene mutations are identified, ∆F508 mutation accounts for
~67% of cases in Caucasians.
• Cystic fibrosis is diagnosed based presence of ↑ sweat chloride concentration,
disease causing CFTR mutations, & symptoms of ≥ 1 associated organ system
↓ Cl- diffusion into peri-ciliary fluid →
↓water composition of peri-ciliary fluid
In children/adults: Distal ileal
obstruction syndrome (DIOS)
↓ reabsorption =
↑secretion of Cl-
into sweat
In GI
tract
↓movement
of intestinal
contents
↓ clearance of mucociliary secretions
In
newborns:
Meconium
ileus
↑ retention of
meconium → ↑
reabsorption of
bilirubin
Prolonged
jaundice in
neonates
↑ Sweat chloride
concentration
Accumulation of secretions in secretory
passages throughout the body,
obstructing these passages
In biliary
tree
Delayed passage of bile →
inflammatory hepatic response
Cirrhosis & portal
hypertension
In upper respiratory tract
In pancreas
Trapped digestive
enzymes degrade
pancreatic tissue
Nasal
polyps
Retained
secretions in
sinuses →
bacterial
proliferation
Pancreas unable to secrete
digestive enzymes into GI tract
(pancreatic insufficiency)
Fat and
protein mal-
absorption
↓ absorption of fat
soluble vitamins
Inflammation →
scarring & fatty
tissue infiltration
→ islet cell
destruction
Chronic
sinusitis
↓ serum Vit. D
Type II Diabetes
Mellitus
Failure to
thrive
Osteoporosis
Published January 21, 2013 on www.thecalgaryguide.com
In lower respiratory tract
Chronic
productive
cough
Retained secretions in airways → bacterial proliferation
à Airway infection & inflammation
Persistent respiratory tract infections
Can progress to chronic bronchitis ± bronchiectasis
(This is the biggest cause of death in CF)
Pathophysiology Signs of obstructive lung dx: i.e.
Lung hyperinflation (on x-ray),
Abnormal pulmonary function
tests
Mechanism
Sign/Symptom/Lab Finding Complications")