SEARCH RESULTS FOR: sickle
central-retinal-artery-occlusion-pathogenesis-and-clinical-findings
 (i.e. Valvular, arrhythmias, congenital defects) (i.e. OCP, Protein C&S deficiency, ATIII deficiency) (i.e. leukemia/lymphoma, sickle cell, polycythemia) Endothelial cell damage Abnormal blood flow 1` coagulation and/or 1 blood viscosity and creates hypercoagulable state causing localized stasis 4, anti-coagulation inflammation
Abbreviations: • GCA — Giant Cell Arteritis • SLE — Systemic Lupus Erythematosus • GPA — granulomatosis with polyangitis • OCP — Oral contraceptive pill • ATIII — Anti-thrombin Ill
Thrombus formation
Blockage of central retinal artery
Central Retinal Artery Occlusion (CRAO)
Authors: Graeme Prosperi-Porta Reviewers: Stephanie Cote Usama Malik Johnathan Wong* * MD at time of publication Carotid Artery Atherosclerosis
Atherosclerotic plaque dislodges from carotid artery
The retina becomes pale 4, perfusion of retinal Slow retinal artery blood Acute retinal edema Ganglion cells and axons from NI, perfusion arterioles due to upstream flow allows for caused by ischemia results death due to ischemia CRAO segmentation of the blood column in a blurred appearance of the retina results in disc pallor seen months after CRAO The choroidal vessels supplying the macula via the posterior ciliary artery become more prominent within a background of retinal pallor")
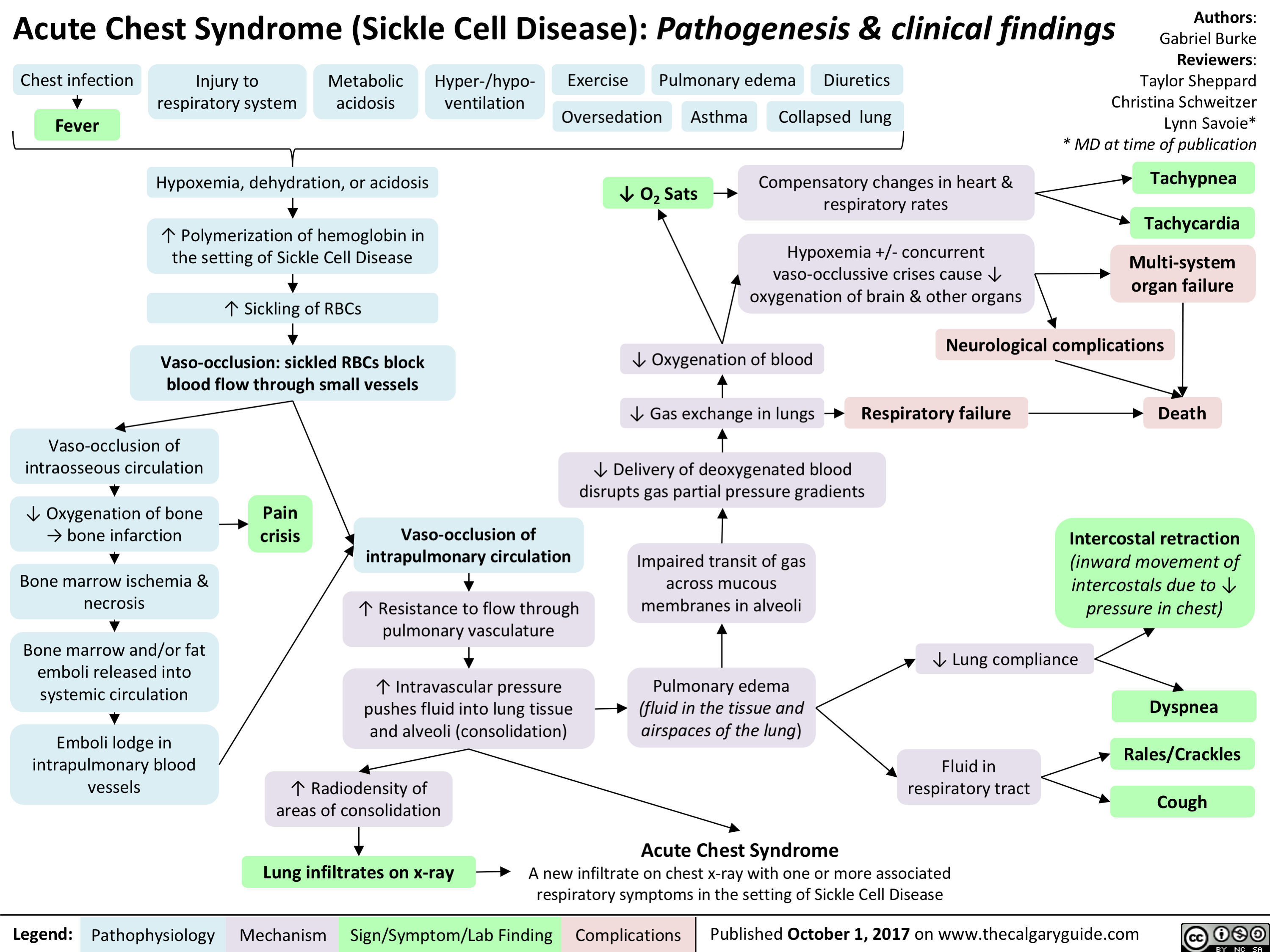
Acute Chest Syndrome (Sickle Cell Disease)
Hemolytic Anemia - Pathophysiology
 may result in slightly macrocytic anemia (because reticulocytes have larger volumes than RBCs)
Defects in the RBC’s environment
Defects in RBC membranes
Ex. Hereditary Spherocytosis:
mutation causing deficiency of RBC structural proteins like ankyrin or spectrin
RBC membranes become weakened and form blebs that break off
↓ RBC surface area while volume remains constantà RBC becomes spherical
Spherocytes in spleen trapped and phagocytosed by splenic macrophages (extravascular hemolysis)
Defects in RBC internal contents (thalassemia, hemoglobinopathies, and metabolic defects)
Ex. Sickle Cell Disease: point mutation in hemoglobin (Hgb) structure (GluàVal)
Inappropriate Hgb polymerization in low oxygen environments due to mutationàRBC becomes rigid, forms a sickle shape
Inflexible RBCs become trapped in the spleen’s sinusoid membranes àphagocytosed by splenic macrophages (extravascular hemolysis)
Infection triggers immune system activation
Autoimmune processes
TTP/HUS (abnormal platelet aggregation blocking blood vessels)
Production of abnormal
antibodies and immune complexes targeted against RBC surface antigens
Immunoglobulin-bound RBCs are marked for
destruction by the immune system (by either the cell- mediated or complement- mediated pathways)
DIC (fibrin deposition blocking blood vessels)
Artificial heart valve
RBCs are sheared when they flow past an abnormal surface
Rate of hemolytic RBC destruction > rate of bone marrow RBC synthesis (reticulocytosis)
↓ total number of RBCs in the body (despite normal RBC production/volume)
Normocytic anemia
Authors: Yan Yu Katie Lin Man-Chiu Poon* Reviewers: Andrew Brack Julia Heighton JoyAnne Krupa Lynn Savoie* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Priapism
 pathways
Post-cavernosal venous drainage is mechanically obstructed e.g. sickle cell disease, dialysis etc.
Ischemic (Low-flow):
Inadequate venous function
Blood pools in corpora cavernosa
Cavernosal cell metabolism uses O2 and releases CO2 into pooled blood
Trabecular smooth muscle relaxes
Cavernosal artery smooth muscle relaxes
Lack of norepinephrine action on penile SM
Post-cavernosal venules are compressed against tunica albuginea
Trabecular smooth muscle and cavernosal artery smooth muscle do not contract
↑ pressure in corpora
↑PCO2 ↓pH
Acidosis
↓PO2
Tissue hypoxia
Tissue damage
Irreversible fibrosis leading to erectile dysfunction
Priapism
Prolonged erection lasting more than 4 hours; in absence of sexual stimulation; not relieved by ejaculation
Trauma to penis or adjacent areas
Authors:
Arsalan Ahmad
Reviewers:
Alec Mitchell
Darren Desantis*
Yan Yu*
* MD at time of publication
Cavernosal artery is damaged
Excessive, unregulated arterial blood flow into corpora cavernosa
Pain
Non-ischemic (High-flow):
Uncontrolled arterial flow
↑ volume of blood in corpora
↑ pressure in corpora
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 22, 2019 on www.thecalgaryguide.com")
急性胸部综合征镰状细胞贫血发病机制和临床表现
:发病机制和临床表现")
Sickle Cell Disease Pathogenesis Clinical Findings and Complications
 Liu Priyanka Grewal Reviewers: Alexander Arnold Luiza Radu JoyAnne Krupa Yan Yu* Lynn Savoie* * MD at time of publication
Hemoglobin S (HbS) variant formed instead of normal Hemoglobin A (HbA)
Hb electrophoresis shows approximately 45% HbS, 52% HbA (ααββ), 2% HbA
Hb electrophoresis shows approximately 90% HbS, 8% HbF, & 2% HbA .
No HbA present
(ααδδ), & 1% HbF (ααγγ;2 fetal hemoglobin)
Heterozygous: point mutation in one of the two chromosomes (Hb AS)
Sickle cell trait
(asymptomatic unless severely hypoxic)
Homozygous: point mutation in both chromosomes (Hb SS)
Sickle cell disease
An inherited blood disorder characterized by defective hemoglobin that leads to red blood cells sickling
2
Dehydration Hypoxemia
Acidosis
↓ Volume of RBC cytoplasm
↓ O2 Saturation of Hb
O morereadily 2
released from Hb in low pH environment
↑ Concentration of deoxygenated HbSinred blood cells (RBCs)
Hydrophilic glutamate→ hydrophobic valine substitution makes HbS less soluble in the cytoplasm & more prone to polymerization & precipitation in its deoxygenated state
↑ Concentration of deoxygenated Hb in RBC leads to ↑ polymerization rate Polymerized & precipitated HbS forms long needle-like fibers
RBC shape becomes sickled
Sickle cells on peripheral blood smear
Vaso-occlusion
(sickled RBCs lodge in small vessels, blocking bloodflow to organs & tissues)
Blockage of venous outflow
Occlusion of vessels in lungs ↑ pulmonary blood pressure
Fluid extravasates into interstitial tissue leading to pulmonary edema
Acute chest syndrome (chest pain, hypoxemia (↓blood oxygen), etc.)**
to the penis:
to the spleen:
Priapism (persistent, painful erection)
Splenic Sequestration (blood pools in spleenà splenomegaly & hypotension)
Extravascular hemolysis (macrophages in the spleen phagocytose sickled RBCs)
Normocytic anemia
↑Marrow erythropoiesis (RBC production) to compensate for hemolysis
Infarction of bone
Pain crises
If occurring in hands
Dactylitis (inflammation of digits)
Blockage of arteries ↓ oxygenation of organs & tissues
Vaso-occlusion of the splenic artery
Splenic infarction (↓ blood supply leads to tissue death)
RBC inclusions (structures found in RBCs) not removed by spleen
Howell-Jolly bodies (RBC DNA remnants) on blood smear
Vaso-occlusion of other arteries (cranial, renal, etc)
Stroke, renal failure
↑ RBC breakdown
↑ Unconjugated bilirubin released from RBC breakdown
RBC precursors (reticulocytes) are released into the blood stream
Reticulocytosis (increased number of immature red blood cells) on peripheral blood smear
Patient’s RBC level becomes dependent on increased marrow activity
Bone marrow infarction or viral infections (i.e. Parvovirus B19) suppresses bone marrow activity
Aplastic crises (profound anemia)
** See corresponding Calgary Guide slide(s)
↑ Serum level of unconjugated bilirubin
Some of the circulating unconjugated bilirubin deposits in the skin
Jaundice (yellowing of skin)
↑ Conjugation of bilirubin in liver
↑Amounts of conjugated bilirubin released into bile
Gallstone formation
Cholelithiasis (presence of gallstones in the gallbladder)
Spleen releases invasive encapsulated bacteria (eg. Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis) into circulation, which causes infections
Meningitis
Sepsis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 16, 2013, updated Apr 29, 2024 on www.thecalgaryguide.com")
Unconjugated Hyperbilirubinemia
 factor
incompatibility
Maternal sensitization
against Rh-positive fetal cells
Maternal antibodies against Rh
factor attack fetal RBCs
ABO incompatibility
Native maternal antibodies against non-
native blood types attack fetal RBCs
Sepsis** Widespread systemic inflammation Cytokines & complement factors damage RBC membranes
Disseminated intravascular
coagulation** (clotting
proteins become overactive)
Clots form in
systemic circulation
Small clots shear & damage
RBCs in circulation
Red blood cell
(RBC) enzyme
defects
Glucose-6 phosphatase
dehydrogenase (G6PD)
deficiency**
G6PD protects RBCs against
oxidative damage
↑ RBC sensitivity to oxidative
stress (during acute stressors)
Pyruvate kinase
deficiency (PKD)
Abnormal glycolysis & cellular
energy production
↓ RBCs life spans
RBC membrane
defects
Hereditary spherocytosis
RBCs are abnormally round (spherocytes)
RBC
membranes
easily damaged
in circulation
Bilverdin reductase
Hereditary elliptocytosis
RBCs are abnormally elongated or oval
converts bilverdin to
Sickle cell
Abnormal hemoglobin (HbS)
RBCs become abnormally
unconjugated bilirubin
disease**
polymerizes under ↓ O2
sickle shaped
Hemoglobinopathies
Thalassemia's**
Defective hemoglobin
chains in RBCs
Irregularly
shaped RBCs
trapped in
spleen
RBC
sequestration
↑ Production of RBCs (Polycythemia**)
Accumulation of blood (i.e.
Cephalohematoma, hemorrhage)
↑ RBC load &
turnover
Causes of ↓
hepatocellular
bilirubin clearance
Genetic defects in
uridine diphosphate
glucuronosyltransfe
rase (UGT) enzyme
(conjugates
bilirubin in liver)
Gilbert syndrome
Unconjugated bilirubin
↓ UGT production
remains insoluble & cannot
Crigler–Najjar
be excreted in bile
syndrome Type II
Crigler–Najjar
syndrome Type I
No UGT production
Breast milk jaundice Breast milk contains β-glucuronidase
Causes of ↑
entero-hepatic
bilirubin circulation
Intestinal obstruction
Obstruction blocks bile flow from liver to intestines Breastfeeding
jaundice
Inadequate milk intake (volume
depletion/dehydration)
↑ Reabsorption of bilirubin
in the intestines
**See corresponding Calgary Guide slide
Legend: Macrophages engulf
old or damaged RBCs
in spleen & liver
↑ Hemolysis (RBC
breakdown)
RBCs release cellular
contents including heme
(from hemoglobin)
Heme oxygenase
converts heme to
bilverdin
↑ Unconjugated
(indirect) bilirubin
accumulation in blood
↑ Total serum
bilirubin levels
Excess bilirubin
deposition into elastin-
rich tissues (eg. skin,
sclera) due to ↑
affinity for elastin
Pathologic neonatal jaundice
(yellow discoloration of skin
within first 24 hours of life)
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published July 13, 2025 on www.thecalgaryguide.com
Authors:
Merry Faye Graff
Khushi Arora
Reviewers:
Annie Pham
Emily J. Doucette
Danielle Nelson*
* MD at time of publication
Hemolytic
anemia**
↓ Bilirubin
conjugation
β-glucuronidase deconjugates bilirubin
Bilirubin builds up
in hepatic system
Unconjugated
bilirubin crosses
blood-brain barrier
Bilirubin-induced
neurologic
dysfunction (BIND)
Kernicterus (bilirubin-
induced neurological
damage)
Scleral icterus
(yellowing of
sclera in eyes)")