SEARCH RESULTS FOR: obstruction
lower-urinary-tract-infections-complications
, stagnant
urine (anatomical variant, obstruction,
neurogenic bladder, urinary reflux)
Bacterial entry (Less Common):
Indwelling catheter, surgical inoculation,
hematogenousspread, trauma
(Staphylococcus, Enterococcus, Candida)
Fecal bacteria access urethra
(E. coli, Proteus, Klebsiella)
Impairment of body's natural defense
systems, or stagnant urine, allow for
bacterial accumulation
Portal of entry bypasses body's physical
defenses (gravity and repetitive outward
urine flow)
Bacterial fimbriae and pili allow
them to ascend urethra and
adhere to epithelium
Lower Urinary Tract Infection (LUTI): Pathogenesis and clinical findings
Suprapubic
Tenderness
Bacterial colony irritates
urinary epithelium
Urgency:
Sensation of need to urinate
quickly or impending
incontinence
Stimulation of
inflammatory
response
Stimulation of urinary reflex
Pathogens use
enzymes to reduce
nitrate to nitrite
Delirium in Elderly
Frequency:
Repetitive need to
urinate
Unique response of altered fluid
status, electrolytes and mental
status, likely as a result of
increased inflammatory cytokines
Lower Urinary Tract Infection (“Cystitis”):
Infection of bladder or distal tract by capable bacteria
colonizing epithelium and causing symptoms
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published March 16, 2014 on www.thecalgaryguide.com
Author:
Brett Edwards
Reviewers:
Riley Hartmann
Jan Rudzinski
Haotian Wang
Steve Vaughan*
* MD at time of publication
Usual Pathogens (“KEEPS”):
K – Klebsiella
E – E. coli (90%)
E – Enterococcus, Enterobacteriaceae
P – Proteus, Pseudomonas
S – Staph. saprophyticus, Serratia
Urine Findings:
↑ Colony Count (>107 CFU/L)
↑ WBC (>10 WBC/μL)
(+) Bacterial culture
(+) Nitrites, Leukocyte Esterase
(+) Foul, turbid urine
+/- Hematuria (rare)")
lower-urinary-tract-infection-pathogenesis-and-clinical-findings
, stagnant
urine (anatomical variant, obstruction,
neurogenic bladder, urinary reflux)
Bacterial entry (Less Common):
Indwelling catheter, surgical inoculation,
hematogenousspread, trauma
(Staphylococcus, Enterococcus, Candida)
Fecal bacteria access urethra
(E. coli, Proteus, Klebsiella)
Impairment of body's natural defense
systems, or stagnant urine, allow for
bacterial accumulation
Portal of entry bypasses body's physical
defenses (gravity and repetitive outward
urine flow)
Bacterial fimbriae and pili allow
them to ascend urethra and
adhere to epithelium
Lower Urinary Tract Infection (LUTI): Pathogenesis and clinical findings
Suprapubic
Tenderness
Bacterial colony irritates
urinary epithelium
Urgency:
Sensation of need to urinate
quickly or impending
incontinence
Stimulation of
inflammatory
response
Stimulation of urinary reflex
Pathogens use
enzymes to reduce
nitrate to nitrite
Delirium in Elderly
Frequency:
Repetitive need to
urinate
Unique response of altered fluid
status, electrolytes and mental
status, likely as a result of
increased inflammatory cytokines
Lower Urinary Tract Infection (“Cystitis”):
Infection of bladder or distal tract by capable bacteria
colonizing epithelium and causing symptoms
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published March 16, 2014 on www.thecalgaryguide.com
Author:
Brett Edwards
Reviewers:
Riley Hartmann
Jan Rudzinski
Haotian Wang
Steve Vaughan*
* MD at time of publication
Usual Pathogens (“KEEPS”):
K – Klebsiella
E – E. coli (90%)
E – Enterococcus, Enterobacteriaceae
P – Proteus, Pseudomonas
S – Staph. saprophyticus, Serratia
Urine Findings:
↑ Colony Count (>107 CFU/L)
↑ WBC (>10 WBC/μL)
(+) Bacterial culture
(+) Nitrites, Leukocyte Esterase
(+) Foul, turbid urine
+/- Hematuria (rare)
WBCs onsite
release enzymes
Cytokines released
systemically
Fever, Malaise,
↑WBC
(>11 x 109 cells/L)
(Rare in LUTI)")
localized-pitting-edema

Authors: Sunny Fong Reviewers: Joseph Tropiano Adam Bass* * MD at time of publication
Central vein thrombosis
Deep vein thrombosis
T in venous pressure is transmitted to the capillaries
1` in capillary hydrostatic pressure
T in fluid extravasation from plasma into the interstitial space distal to site of obstruction or insufficiency
Localized Pitting Edema: Edema fixed at a specific anatomical site
Venous obstruction causes'` blood pooling distal to site of obstruction
Starling's Equation:
Net filtration gradient = LpS x ((Pap — Pint) Olcap
LpS = Porosity or permeability of the endothelial layer Pup = Capillary hydrostatic pressure Pint = Interstitial hydrostatic pressure ncap = Capillary oncotic pressure flint = Interstitial oncotic pressure
Note: An increase in net filtration gradient (eg. Increased capillary hydrostatic pressure or decreased capillary oncotic pressure) can lead to the formation of edema")
pathogenesis-of-select-causes-of-constipation-in-adults-and-in-elderly
 Hypercalcemia) Hypothyroid-ism) Sclerosis) Scleroderma) Analgesics)
Mechanical I`Ca2+ = 4, Na+ Thyroid Demyelination Collagen Puborectalis Disturbance in obstruction in permeability in hormone of CNS neurons deposits into muscle and the gut-brain the bowel neurons deficiency colonic mucosa, leading to external anal sphincter fail interaction fibrosis of the gut wall to relax Interrupted 4, Excitability Possible Dysfunction of Narrowed Mechanism flow of bowel contents and tone of bowel smooth mechanisms: hormone autonomic nerves that anorectal angle and unknown, many Atrophy of the muscle receptor supply smooth muscle '`pressure of pathways changes, involuntary wall of the colon anal canal neuromuscular disorders, myopathy from bodily functions 1, Peristalsis of infiltration of 4, Ability of the Evacuation Visceral the bowel colon to contract of feces is hypersensitivity Abbreviations: the intestinal wall 4, Digestion less effective and 4, colonic and colonic motility motor • IBS-C: Irritable Bowel Syndrome with predominant constipation • CNS: Central Nervous System 4, Peristalsis of response after a meal the bowel
Opioids bind to Lt-opioid receptors on gut wall
Inhibition of excitatory neural pathways within the enteric nervous system
1, Peristaltic contractions
1
l• Colonic transit time")
Pituitary Mass Effects
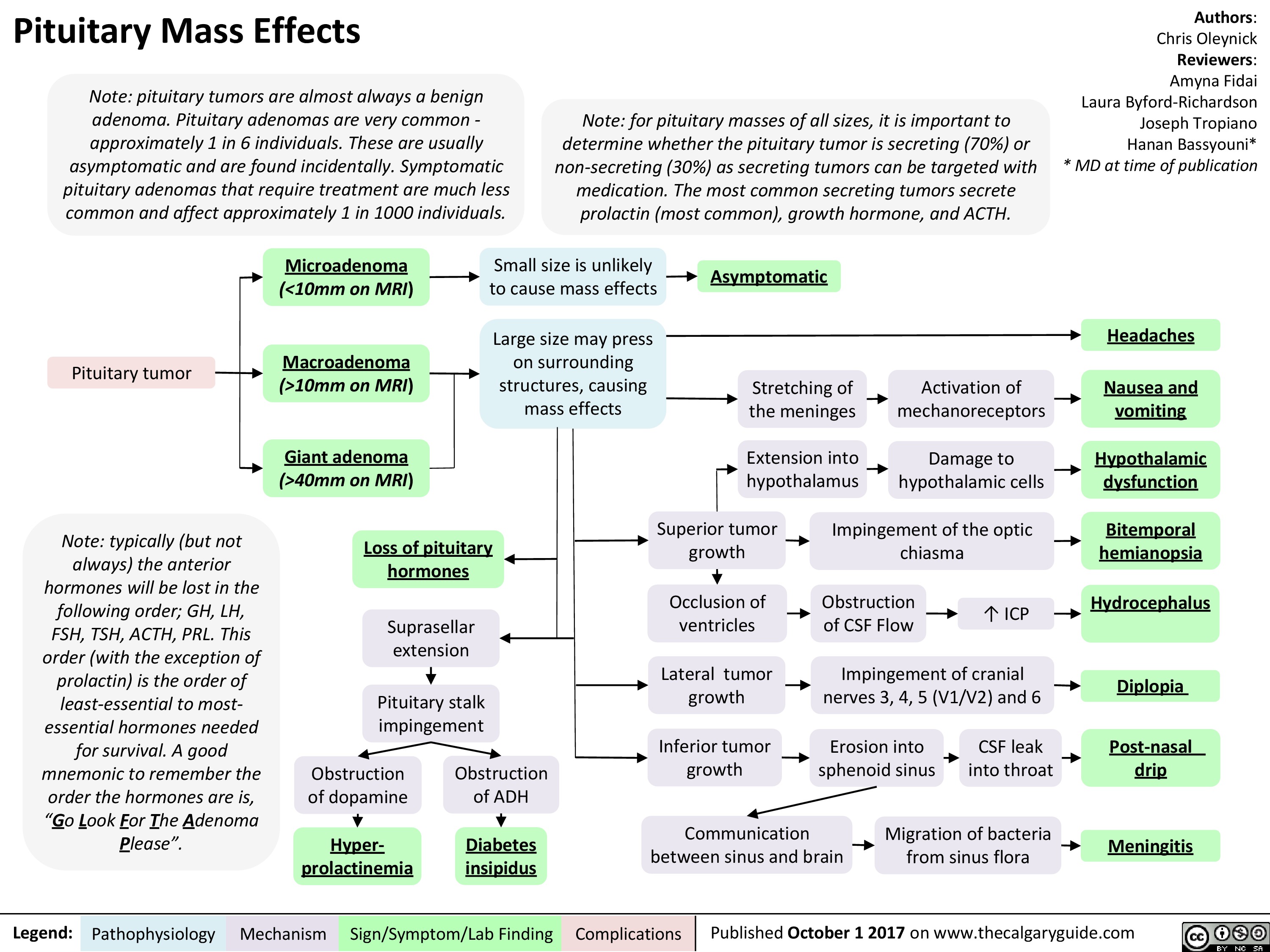 10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" title="Pituitary Mass Effects
Note: pituitary tumors are almost always a benign adenoma. Pituitary adenomas are very common -approximately 1 in 6 individuals. These are usually asymptomatic and are found incidentally. Symptomatic pituitary adenomas that require treatment are much less common and affect approximately 1 in 1000 individuals.
Pituitary tumor
Note: typically (but not always) the anterior hormones will be lost in the following order; GH, LH, FSH, TSH, ACTH, PRL. This order (with the exception of prolactin) is the order of least-essential to most-essential hormones needed for survival. A good mnemonic to remember the order the hormones are is, "Go Look For The Adenoma Please".
Legend:
Note: for pituitary masses of all sizes, it is important to determine whether the pituitary tumor is secreting (70%) or non-secreting (30%) as secreting tumors can be targeted with medication. The most common secreting tumors secrete prolactin (most common), growth hormone, and ACTH.
Authors: Chris Oleynick Reviewers: Amyna Fidai Laura Byford-Richardson Joseph Tropiano Hanan Bassyouni* * MD at time of publication
Microadenoma Small size is unlikely to cause mass effects (<10mm on MRI) Asymptomatic Macroadenoma Large size may press on surrounding structures, causing mass effects Headaches Stretching of the meninges Activation of mechanoreceptors Nausea and (>10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" />
10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" title="Pituitary Mass Effects
Note: pituitary tumors are almost always a benign adenoma. Pituitary adenomas are very common -approximately 1 in 6 individuals. These are usually asymptomatic and are found incidentally. Symptomatic pituitary adenomas that require treatment are much less common and affect approximately 1 in 1000 individuals.
Pituitary tumor
Note: typically (but not always) the anterior hormones will be lost in the following order; GH, LH, FSH, TSH, ACTH, PRL. This order (with the exception of prolactin) is the order of least-essential to most-essential hormones needed for survival. A good mnemonic to remember the order the hormones are is, "Go Look For The Adenoma Please".
Legend:
Note: for pituitary masses of all sizes, it is important to determine whether the pituitary tumor is secreting (70%) or non-secreting (30%) as secreting tumors can be targeted with medication. The most common secreting tumors secrete prolactin (most common), growth hormone, and ACTH.
Authors: Chris Oleynick Reviewers: Amyna Fidai Laura Byford-Richardson Joseph Tropiano Hanan Bassyouni* * MD at time of publication
Microadenoma Small size is unlikely to cause mass effects (<10mm on MRI) Asymptomatic Macroadenoma Large size may press on surrounding structures, causing mass effects Headaches Stretching of the meninges Activation of mechanoreceptors Nausea and (>10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" />
Ischemia: Pathogenesis of Cellular Injury and Death

Bronchogenic Carcinoma - Pancoast Tumors Pathogenesis and clinical findings

Endothoracic fascia
1— Parietal pleura •
1—
Upper ribs
Large Cell
Carcinoma
Adenocarcinoma
Squamous Cell
Carcinoma
Primary Bronchogenic
Carcinoma
Pancoast tumor:
Local/metastatic growth in
ipsilateral lung apex
Disruption of structures
adjacent to superior
pulmonary sulcus
NSCLC (more common)
Invasion of airways
► causing obstruction
(later stages)
Author:
Bradley Stebner
Daniel Meyers
Midas (Kening) Kang
Reviewers:
Natalie Morgunov
Sadie Kutz
Usama Malik
Kerri Johannson*
*MD at time of publication
Notes:
• Pancoast Tumor: Malignant
lesion occupying the superior
pulmonary sulcus (lung apex)
Bronchogenic carcinoma:
primary malignant neoplasm
arising from epithelium of
bronchus or bronchiole
Pancoast tumors can be caused
by primary or metastatic
pulmonary neoplasms
(described here) as well as
infectious foci
Hemoptysis
Compression of C8
and T1 nerves
•
Disruption of paravertebral
sympathetic chain
Shoulder • Weakness in intrinsic Horner's • 4, sympathetic to to iris muscle Syndrome 4, sympathetic radial to eccrine sweat gland
Pain (ulnar hand muscles
nerve) 4, sympathetic innervation STM
Paresthesia in
4th /5th digits and
arm/forearm medial
Ptosis Mi o sis Anhidrosis Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Compression of SVC
SVC Syndrome
•
4, venous return to
RA
4, Cardiac output to
lungs
Dyspnea
Disruption of RLN
1
Hoarse voice
4, venous drainage
from upper thoracic
cavity
Retention of fluid in
upper limb
•)r
Facial and limb swelling")
Asthma Acute Exacerbation: Pathogenesis and Treatment
: An episode of increased symptoms due to decreases in airflow
Abbreviations • PCO2: Partial pressure of CO, in arterial blood • PEF: Peak expiratory flow • SABA: Short-acting beta-2 agonists • Sp02 : Blood oxygen saturation level
Mild to moderate exacerbation: PEF 50% of predicted
Titrate O2 toSpO2, 92%, give SABA & steroids ■
Good response: symptoms resolved, PEF > 80%
[Treat at home with SABA as needed and steroids
Dyspnea
Bronchoconstriction
1` Residual volume and 1` PCO2
Respiratory failure
1` Air trapping causes '1' intra-alveolar pressure
Severe exacerbation: PEF 50% of predicted Educate patient regarding medications, Loss of Pulsus inhaler technique & [consciousness paradoxus follow up with primary care provider I
Legend: Pathophysiology Mechanism
Titrate O2 to402 93%, give SABA, steroids & magnesium sulfate
Sign/Symptom/Lab Finding
{Worsening symptoms and/or respiratory failure: Do not delay intubation, send to ICU, give SABA, steroids & magnesium sulfate
Authors: Luke Gagnon Reviewers: Midas (Kening) Kang Usama Malik Lian Szabo* * MD at time of publication
4, Delivery of oxygen rich air to alveoli 4, Oxygenation of blood
Drowsy and confused
Central cyanosis
• Tachycardia
Pneumothorax
[Depending on 1 severity: Observation or place chest tube")
Bronchiectasis Pathogenesis and clinical findings
, MAC complex infection, COPD, allergic bronchopulmonary aspergillosis, chronic infections
Irreversibly dilated bronchi
Chronic bronchial infection and inflammation
1
Easily collapsible airways
I Bronchiectasis (persistent and progressive damage to lungs)
Chronic cough (mucopurulent)
Defect in immunity and/or mucus clearance
Persistent bacteria in airway (commonly Pseudomonas/Staph aureus)
Inflammatory response
Rhinosinusitis
Abbreviations: • A1AT — Alpha-1-antitrypsin • COPD — Chronic Obstructive Pulmonary Disease • HIV — Human Immunodeficiency Virus • MAC — Membrane Attack Complex • VQ— Ventilation/Perfusion ratio
Legend:
Pathophysiology Mechanism
Fever
Sign/Symptom/Lab Finding
Failure to thrive (children)
Authors: Rebecca (Becky) Phillips Reviewers: Midas (Kening) Kang Usama Malik Eric Leung* * MD at time of publication
Notes: • Can be focal (single lobe/segment) or diffuse (both lungs) • Mainly in elderly • 1% prevalence in children
Tissue damage
Epithelial destruction of airways
Further impairment of bacterial clearance
Persistent inspiratory adventitious sounds (crackles > wheezing)
Complications
Structural damage to bronchial walls
Obstructive pulmonary function tests
Hemoptysis
Chest pain
VQ mismatch and 4, gas exchange
4, oxygenation
Digital clubbing (rare)
Fatigue Dyspnea
Cyanosis (uncommon)")
Lung cancer clinical findings and paraneoplastic syndromes

Obstruction of proximal airway
Inability to clear inhaled pathogens Postobstructive pneumonia
Cough, fever, dyspnea
Local tumor growth
Spread of tumor to pleural surface
Chest Pleural discomfort effusion
• Obstruction or compression at local site
Uncontrolled abnormal cell growth in one or both lungs 4 Lung Cancer
Airway invasion
Hemoptysis
Lambert-Eaton syndrome (Production of auto-antibodies against Calcium channels)
Muscle weakness
I` effort to Compression at the Compression Superior vena ventilate the laryngeal nerve of brachial cava lungs nerve plexus compression Impaired innervation to the vocal cords Dyspnea Shortness of Arm/shoulder/ Face/arm breath Voice hoarseness neck pain edema
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Authors: Yoyo Chan Reviewers: Midas (Kening) Kang Usama Malik Leila Barss* * MD at time of publication
Tumor secretes biologically active substances
Paraneoplastic Syndromes 4 Associated symptoms with malignant diseases
TGF131 extracellular matrix protein
Fingers clubbing
PTHrP T calcium release from bones
Hypercalcemia Serum calcium >2.6 mmol/L
ADH 1 SIADH T water reabsorption 1
Hyponatremia Serum sodium <135mEq/L
Abbreviations: • ACTH: Adrenocorticotropic hormone • ADH: Anti-diuretic hormone • PTHrP: Parathyroid hormone-related protein • SIADH: Syndrome of inappropriate antidiuretic hormone production • TGFI31: Transforming growth factor beta 1
1` ACTH
cortisol release and production
Cushing's syndrome (symptoms and signs caused by prolonged cortisol exposure)
Muscle weakness, hyperglycemia, severe hypokalemia")
Benign Prostatic Hyperplasia: Pathogenesis and medications

Note: MoA not fully established
PDE-5 inhibitors (e.g. tadalafil)
Bladder and prostate smooth-muscle a-1 receptor antagonism
—110.
Relaxation of bladder outlet and prostate smooth-muscle
Authors: Michael Korostensky Reviewers: Alex Tang Usama Malik Dr. Jay Lee* * MD at time of publication
Acronyms: 5-ARI = 5-a reductase inhibitors COX = cyclooxygenase DHT = dihydrotestosterone GnRH = gonadotropin-releasing hormone LUTS = lower urinary tract symptoms PDE-5-mediated cGMP degradation in prostate smooth-Improved urinary outflow muscle and associated vascular supply Relaxation of prostate smooth-muscle MoA = mechanism of action NSAID = nonsteroidal anti-inflammatory drugs PDE-5 = phosphodiesterase-5 -NO
5-ARIs (e.g. dutasteride)
LHRH receptor antagonists (e.g. cetrorel ix)
P3-adrenergic agonists (e.g. mirabegron)
anticholinergics (e.g. oxybutynin)
NSAIDs
1` Bladder pressures
Pathophysiology Mechanism
5-a-reductase activity
1, Conversion of testosterone into DHT
4, Progression of LUTS
1, Testosterone secretion from testicular Leydig cells 1, LH secretion from pituitary GnRH antagonism DHT production Relaxation of detrusor Bladder muscle 1` capacity Improved LUTS
Acetylcholine antagonism at muscarinic receptors Relaxation of bladder outlet smooth-muscle 1` volume to first detrusor contraction 4, Prostaglandin release Analgesia and 4, Prostatic ,f, COX activity ► inflammation —110. Bladder smooth-muscle hyperplasia (detrusor thickening) /1` Sensitivity (i.e. overactive detrusor) -1110. 1, Volume to first detrusor contraction LUTS")
Mixed Urinary Incontinence Pathogenesis and clinical findings
 4, Urinary leakage preceded by a sudden, strong urge to void
Overflow Incontinence vir Overfilling of the bladder from obstruction; BOO (tumour, stone, BPH, urethral or bladder neck stricture)
Detrusor Overactivity Ilr OAB (idiopathic), CNS lesion (neurogenic), inflammation/ infection (cystitis, UTI), diabetes mellitus
4. Bladder Wall Compliance
Progressive t in intravesicle pressure during bladder filling pushing urine from the bladder
Authors: Braden Millan Reviewers: Alex Tang Usama Malik Jay C. Lee* * MD at time of publication
Stress Urinary Incontinence (SUI) + Episodic involuntary urinary leakage with sudden l• in intra-abdominal pressure
4.
Urethral hypermobility, intrinsic sphincter deficiency, or a poorly coapting urethra
4,
4, Pelvic floor muscle and ligament strength causing 4. tone of vesicoureteral sphincter unit; 4, urethral strength and associated striated and smooth muscle; iatrogenic
Legend:
Failure to Void Weak Stream (+ dribbling), Intermittent, Straining, '1` PVR if a complication of urinary retention; obstruction visible on cystoscopy
Failure to Store Frequency, Urgency, Nocturia, Dysuria if SUI or UUI not caused by obstruction
Pathophysiology Mechanism
Urodynamic Studies SUI — 4, urethral closure pressure with 11` IAP/Bladder Volume and urinary leakage UUI — involuntary detrusor contraction and/or detrusor sphincter dyssynergia
Incontinence, 4, Quality of Life, UTI's")
Periorbital Cellulitis: Pathogenesis and Clinical Findings

Note: Also referred to as preseptal cellulitis
Dacryoadenitisa Conjunctivitisb
Acute chalazionc
Dacryocystitisd Hordeolume
Streptococcus pneumoniae, Moraxella catarrhalis, non-typable Haemophilus influenza (most common organisms)
Abrasion Insect bite
Burns Trauma
Local infection
Contiguous spread of infection
Sinusitis
Otitis media Hematogenous spread
Local break in skin Micro-organisms enter
Definitions:
Note:
Eye exam should reveal normal:
- extra-ocular
movements and globe
position
- pupillary reflex and
visual acuity
If any are abnormal, the presentation is no longer considered periorbital cellulitis, as the infection has likely spread beyond the preseptal compartment/orbital septum.
If the eye cannot be assessed, the patient NEEDS a CT scan.
Pathogens reach dermis and subcutaneous periorbital tissue
Periorbital Cellulitis
a. Dacryoadenitis: infection of the lacrimal glands
b. Conjunctivitis: inflammation of the conjunctiva
c. Chalazion: a benign, painless bump or nodule inside the upper or lower eyelid which results from healed internal hordeolums that are no longer infectious.
d. Dacryocystitis: an infection of the lacrimal sac, secondary to obstruction of the nasolacrimal duct at the junction of lacrimal sac.
e. Hordeolum: localized infection or inflammation of the eyelid margin involving hair follicles of the eyelashes or meibomian glands.
Spreads beyond preseptal compartment/orbital septum
Involves the orbit Orbital cellulitis
See slide on Orbital Cellulitis: Pathogenesis and clinical findings
Localized inflammation
Pain on palpation
Induration
Warmth
Eyelid and periorbital edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Sinusitis: Pathogenesis and clinical findings

Vesicoureteric reflux (VUR): Pathogenesis and clinical findings
: Pathogenesis and clinical findings
Authors: Nicola Adderley Reviewers: Emily Ryznar *Lindsay Long * MD at time of publication
Abnormal function
Abnormal anatomy
Neurogenic bladder (e.g. cerebral palsy, constipation, spinal injury, iatrogenic)
Non-neurogenic bladder (neuropsychological)
Lower urinary tract abnormality (posterior urethral valves, meatal stenosis)
Bladder outlet obstruction
↑ pressure distorts UVJ
Upper urinary tract abnormality (ureters)
UVJ abnormality
Incomplete closure of UVJ during bladder contraction
Abbreviations
• UVJ - ureterovesicular junction • UTI – urinary tract infection
Failure of bladder sphincter to relax during bladder contraction
Vesicoureteric reflux (VUR):
Back flow of urine from the bladder into one or both ureters +/- kidneys
Migration of lower urinary tract bacteria to kidneys
Bacterial invasion of renal parenchyma
Upper UTI (pyelonephritis)
Incomplete emptying of bladder during Abnormal
↑ pressure in bladder
Bladder dilates
Dilated bladder on U/S
urination
Bacteria in bladder are not cleared during urination
voiding habits
↑ bladder capacity
Renal scarring
↓ functional renal tissue
*Chronic kidney disease (↓ GFR,
hypertension, proteinuria)
Flank tenderness
Fever, dysuria, urgency, frequency
Lower UTI (cystitis) Urinary stasis
Cloudy, foul- smelling urine
Urethral stricture
Notes
Urgency, dysuria, frequency
• First febrile UTI in an infant should trigger a work-up for VUR
• High likelihood of spontaneous resolution • *Late complication of severe VUR
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com")
Microangiopathic Hemolytic Anemia: Pathogenesis and clinical findings

↓ Inhibition of complement
Immune inflammatory
↑ Pressure in
↑ Extrinsic clotting pathway activation
TTP
(See TTP-HUS Slide)
Disruption of
endothelial cell
activation perfusion/ischemia response metabolism vasculature ↑Thrombin Deficient
Placental under-
renal afferent
↑ Complement pathway activation
MAC-mediated cell lysis
Cytokine release
Endothelial injury
Shear stress on endothelium
production
↑ Fibrin clot production and deposition in small vessels
ADAMTS13 protease enzyme
↓ Cleavage and ↑ accumulation of VWF multimers
Abbreviations:
• HELLP - Hemolysis, Elevated Liver Enzymes, Low Platelets • HUS - Hemolytic-Uremic Syndrome
• DIC - Disseminated Intravascular Coagulation
• TTP - Thrombotic Thrombocytopenic Purpura
• MAC - Membrane Attack Complex
• STEC - Shiga Toxin-Producing Escherichia coli
• VWF - Von Willebrand Factor
Pro-thrombotic Environment (see Virchow’s Triad Slide)
Platelet aggregation Mechanical obstruction of the vessel lumen
Hypercoagulable state
Thrombocytopenia
↑ RBC production in bone marrow
↑ Reticulocytes
Hemoglobin released from damaged RBCs Shearing of RBCs Anemia
Binds to haptoglobin Conversion to bilirubin in liver
↓ Free haptoglobin ↑Indirect bilirubin
Shistocytes Jaundice
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 13, 2018 on www.thecalgaryguide.com")
Venous insufficiency- Signs and symptoms

Biliary Atresia (BA)- Pathogenesis and clinical findings
- Pathogenesis and clinical findings Intrauterine environment genetic factors abnormal bile duct development toxic inflammatory response viral immunologic injury to bile duct epithelia pathophysiology poorly understood histology consistent with obstruction on liver biopsy biliary atresia progressive idiopathic fibre-obliterative disease extra-hepatic biliary tree biliary obstruction on intra-operative cholangiogram (diagnostic) partial complete bile duct obstruction delivery of bile acids to small intestine pressure in bile duct absorption of fat and soluble vitamins vitamin K+ deficiency coagulopathy INR PTT bruising petechiae acholic pale stool failure to thrive elimination of bilirubin conjugated direct bilirubin jaundice pruritus excreted urine dark urine diaper yellow pressure bile duct GGT backs up in liver cholestatic hepatitis firm enlarged liver fibrosis cirrhosis ALT AST Horwitz Adderley McKenzie")
Crohn's Disease

Inflammation of the GI tract lining
- Inflammation is “transmural”, spanning the entire thickness of the intestinal wall from luminal mucosa to the serosa.
- The inflammation occurs anywhere in the GI tract from the oral mucosa to the anal mucosa (from ‘gums to bum’) in skip lesion pattern.
Atrophy, scarring of the intestinal villi
Inflammatory cytokines destroy the mucosa epithelial cells of the GI tract wall, causing cell apoptosis and ulceration
↑ permeability of the blood vessels supplying the GI tract wall
Chronic inflammation impairs healing responses
Dysregulated wound healingàexcess
extracellular matrix deposition
Fibrosis leads to scar tissue and thickening of all layers of the GI tract
Strictures
Inflammation is systemic, affecting:
Joints Arthropathy Erythema
Impaired absorption of nutrients
Weight loss
Prolonged GI bleeding
Anemia
Transporter proteins responsible for Na+ reabsorption gradually disappear from the epithelium
More sodium (and thus water) is
retained in the GI tract lumen
Microperforations can penetrate through the intestinal wall
Anal fistulae (“holes” connecting the anus to the skin, bladder, peritoneum, small bowel, etc.)
Continued inflammation and/or infection can lead to:
Leakage of fluid out of capillaries into the GI tract
Luminal edema and swelling
Narrowing of GI lumenàbowel obstruction
Skin
Mouth Eyes
Liver
nodosum, pyoderma gangreno- sum
>5 canker sores
Uveitis
Iritis, scleritis
Sclerosing cholangitis
↓ fat absorption
Fatty acids (negatively charged) bind Ca2+, freeing oxalate from Ca2+
↑ oxalate absorbed into blood & filtered by kidney
Calcium oxalate kidney stones
Diarrhea
Abdominal cramping and pain
(see Bowel Obstruction page for full mechanism
Anal abscesses Inflammatory masses
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Signs and Symptoms of Pulmonary Embolism

Deep Vein Thrombosis – popliteal, femoral, iliac veins Clot migrates to IVCàright atrium of heartàright
ventricleàpulmonary vasculature
Large clots (saddle emboli) are lodged in pulmonary arteries
Small clots are lodged in pulmonary arterioles
Saddle embolus (pulmonary artery obstruction)
Back-up of blood into right heart
Right heart strain
↓ CO2 delivery to the lungs for exhalation
Less CO2 exhaled, CO2 builds up in the blood, triggers medullary chemoreceptors to ↑ respiratory rate
Well-ventilated (V) areas of lung do not receive adequate blood supply (Q); vice versa
V/Q mismatch
On V/Q scan
Signals brain to ↑ heart rate
Ischemic tissue becomes inflamed and adheres to pleura
Pleural friction rub
Sandpaper-like sound heard on auscultation
Pleuritic chest pain
Focal, localized chest pain that occurs with each breath
Clot ↓ pulmonary arterial/arteriolar blood flow
↓ delivery of deoxygenated blood to alveoli for oxygenation
Low O2 in blood (↓ O2 saturation) is detected by aortic/carotid chemoreceptors
Signals brain to ↑ respiratory rate
If circulation to lung periphery is cut off, sub-pleural lung tissue can become ischemic and infarct
Irritation of somatic sensory nerve endings on the parietal pleural membrane
Pain stimulates adrenergic response
Tachycardia
Dyspnea/shortness of breath (SOB)
Most sensitive indicator of PE, but not very specific
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Secondary Polycythemia

Poor lung function
Renal artery stenosis
↓ blood flow to kidney
Kidney senses ↓ O2
High affinity Hb or CO poisoning
Hb does not easily unload O2
Tissues become hypoxic
Tumors (e.g. renal, hepatic, lung)
Secretes EPO in an unregulated way, as a “paraneoplastic syndrome”
High altitude
Obstructive sleep apnea
Episodic airway obstruction during sleep
Intermittent hypoxia
Cyanotic heart disease
Shunting of blood
Venous and arterial blood mixes
Poorly oxygenated blood
↓ O2 partial pressure
↑ EPO production independent of O2 (inappropriate response)
↑ EPO production due to hypoxia (appropriate response)
Abbreviations:
• Hb- Hemoglobin
• EPO- Erythropoietin • ILD- Interstitial Lung
Disease
• COPD- Chronic
Obstructive Pulmonary Disease
“Endogenous causes” of high EPO
Secondary Polycythemia
“Exogenous causes” of high EPO
Testosterone therapy Iatrogenic EPO (results in ↑ EPO synthesis administration
within the body)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
Ulcerative Colitis

Immune response against the GI tract. (Unclear mechanism, but thought to be mediated by cytokine release and neutrophil infiltration)
Inflammation of the GI tract epithelial lining
- Starting at the rectum and moves up the colon and is continuous (does not invade the small intestine)
- Inflammation affects the mucosal and submucosal only
Diarrhea, abdo pain and cramping causing avoidance of food
Weight loss
Apoptosis of GI tract mucosa
Transporter proteins responsible for Na+ reabsorption gradually disappear from the epithelium
Ulceration, into the anus, and more severe
Prolonged Bleeding - GI and anus
Anemia, often iron deficiency
Inflammation ↑ permeability of the blood vessels supplying the GI tract wall
Fluid leak out of capillaries into GI tract wall, causes edema and swelling
Swelling narrows the GI tract lumen, causing bowel obstruction
Inflammation, ulceration, or infection at the anus (all involve the RECTUM!)
Anal irritation stimulates autonomic and somatic nerves leading up to the brain, causing the pt to want to defecate
Tenesmus, urgency, frequency (feeling or urgency to defecate, but little stool is produced)
Joints Skin
Arthroplasty/ joint pain
Erythema nodosum, pyoderma gangrenosum
Mouth >5 canker sores
More sodium (and thus water) is retained in the GI tract lumen
Bloody Diarrhea, usually bloody due to anal bleeding and ulceration bleeding
Abdominal Cramping and pain (see Bowel Obstruction page for full mechanism)
Eyes (uvea, iris, sclera)
Liver Blood
Uveitis
Iritis, scleritis
Sclerosing Cholangitis
Autoimmune hemolytic anemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
intraventricular-hemorrhage-in-preterm-infants-clinical-findings-and-complications
 in preterm infants:
Clinical findings and complications
Authors: Alexa Scarcello Reviewers: Nicola Adderley, Emily Ryznar, Yan Yu*, Jennifer Unrau* * MD at time of publication
Volpe Grading Grade I: germinal matrix
hemorrhage with no or minimal IVH (<10% of ventricular area)
Grade II: IVH (10-50% of ventricle) Grade III: IVH (>50% of ventricle;
usually distends lateral ventricle)
Grade IV/Intra-parenchymal echodensity (IPE): periventricular hemorrhagic infarction
Inflammation/dysfunction of arachnoid villi
↓ absorption of CSF 2° to obstruction of arachnoid villi
Communicating hydrocephalus (IVH grades II-IV)
Venous congestion
Venous infarction
Periventricular hemorrhagic necrosis
Destruction of periventricular motor tracts
Cerebral palsy
Rapid significant blood loss
↓ intravascular blood volume
Hypotension
↓ bloodflow to the brain to support brain function
Intraventricular Hemorrhage (IVH)
hemorrhage in periventricular subependymal germinal matrix
Ultrasound: blood in germinal matrix, ventricles, or cerebral parenchyma
Sudden ↓ hematocrit
Blood irritates contiguous structures
Variable neurologic findings; including altered level of consciousness, hypotonia, apnea, etc
Neuro- developmental abnormalities (varying severity)
See slide - Hydrocephalus: Clinical Findings in Pediatrics
This mechanism leads to three different possible clinical manifestations:
1. Silent Presentation (most common)
2. Stuttering/Saltatory Course: non-specific findings - hypotonia, apnea, altered level of consciousness, bradycardia, and ↓ Spontaneous movements
3. Catastrophic Deterioration (least common) Stupor or coma, decerebrate posturing, seizures, bradycardia, metabolic acidosis, bulging fontanelles, abnormal pupillary reflexes, inappropriate ADH secretion
Notes
• Incidence & severity are inversely proportional to gestational age
• 50% occur within 1st day of life, 90% by 3rd day
• As explained in the flow chart, the postnatal clinical presentations of
IVH fall into three categories (1-3)
• Symptoms of catastrophic bleeds are uncommon and usually caused
by rapid significant blood loss with subsequent neurologic findings 2° to meningeal irritation, inflammation, and potential mass effect/acute hydrocephalus; severe bleeds may also occur in the absence of clinical findings attributable to IVH
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 27, 2019 on www.thecalgaryguide.com")
Appendicitis

The appendix is anatomically located in the RLQ; appendicitis may be confused with disorders of surrounding structures: Gynecological Diseases
• RuleoutpregnancywithHCG pregnancy test
• Rupturedovariancyst
• Ectopicpregnancy
• Mittelschmerz(mid-cycle
pain)
Gastro-intestinal Diseases
• Meckel’sdiverticulum (presents identically to appendicitis; surgically located 2 feet from ileocecal valve; mostly seen in children)
• Diverticulitis(presentsasleft sided appendicitis)
Non-GI Abdominal Issues
• Mesentericadenitisinkids <15: swollen mesenteric lymph nodes
• Renalcolic
Obstruction of appendiceal lumen (by fecalith, fibrosis, neoplasia, foreign bodies or lymph nodes in kids)
Appendix distension and spasms
↑ lumen pressure, ↓ blood flow to appendix
Ischemia, tissue necrosis, loss of appendix structural integrity
Bacterial invasion of the appendix wall, causing transmural inflammationandnecrosis
Stretching of visceral peritoneum, stimulation of autonomic nerves T9-T10
Progression of inflammation over several days (variable length of time)
Irritation of parietal peritoneum, stimulation of somaticnerves
If appendix not surgically removed
Perforation of colon wall, causing peritonitis, abscesses or death
Note: Symptoms hugely variable. Only 30% present with classic history. Diagnosis is mostly clinical. Further investigations:
CBC: Leukocytosis (due to inflammatory response) CT: Gold standard test. Thickened visceral membrane with enhancing (white) rim due to ↑ blood flow
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Acute GI Related Abdominal Pain

Bowel stretching, pulling, contracting
Abdominal pain type:
Diffuse, non-localized Dull, crampy, periodic Not associated with movement
Patient may writhe around, trying to get rid of the pain
Mesentery Intestinal lumen
Parietal peritoneum
(innervated by somatic nerves)
Cross-section of the GI tract
Cuts, structural damage, and inflammation in the bowel
Important Notes
• Acute abdominal pain can also result from non-
gastrointestinal causes, such as kidney stones, female reproductive tract issues, and urinary tract issues. For simplicity’s sake, only the GI-related acute abdominal pain disorders are listed here.
• The DDx of visceral abdominal pain is broad. Please consult relevant sections of the Calgary Black Book for the DDx.
• Keep in mind that visceral abdominal pain can also be caused by the “acute abdomen” diseases (if the diseases are presenting in their initial phases).
• • •
• • •
Abdominal pain type:
Sharp, well-localized
Excruciatingly painful, persistent Associated with movement of bowels
Patient often lies still to avoid abdominal vibration
Peritoneal signs
Abdominal guarding, pain with abdominal vibration (coughing, shaking, percussion, palpation)
Transition from diffuse to localized pain can indicate disease progression (e.g. from visceral to parietal peritoneal inflammation)
Note: bowel obstruction may or may not present as acute abdominal pain
Bowel Infarction
Appendicitis Diverticulitis
Acute Cholecystitis
Acute Pancreatitis
Perforated Ulcer
DDx of an “acute abdomen”:
A sudden, non-traumatic disorder of the abdomen that needs urgent diagnosis and treatment. Each topic will be further explored in their respective slides.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Colorectal Carcinoma pathogenesis and clinical findings

↓ appetite
Local bleeding
Abdominal Abscess
Weight loss
Acute blood loss
Iron deficiency anemia
Classification of tumours/abnormal growths:
1. Adenoma–abenigntumorfromglandular structures
2. Carcinoma–cancerarisingfromtheepithelial tissue of the skin or the lining of internal organs
3. Sarcoma–cancerarisingfromconnectivetissue
Mechanical bowel Obstruction
Ribbon (thin) stool
In rectum
Mass effect
Tumor ↓ bowel lumencaliber
Backed up contents mayberegurgitated
Cancerinvadesrectal sphincters, muscles, vessels&nerves
Compressing ureters, urine backs up into kidney
Compressing stomach
Abdominal distension/pain Invades blood vessels
Inflammatory
Bowel Disease Smoking
Abdominal radiation
Tubular adenomas
(pre- cancerous polyps)
Obesity
Local growth of tumor
Cell line mutations
Idiopathic
Uncontrolled cell division in the colon and rectum
Hereditary syndromes
Colorectal Carcinoma
(Develops over time)
Outside bowel serosa
Bowel perforation
Bowel to bowel/local organ fistulisation
Host immune cells release cytokines to combat cancer
Bowel contents leak
Metabolic abnormalities, ↑energy use
Tumor Spread Mechanisms:
1. Hematogenous 2. Lymphatic
3. Contiguous
4. Transperitoneal
Tumor cells spread distally
Friable vessels supply tumor
Metastatic Disease
Vessels Rupture
Occult bleeding &
melena (black stools) depletes stores of iron
Authors:
Karly Nikkel
Reviewers:
Michael Blomfield
Tony Gu
Yan Yu*
Edwin Cheng*
* MD at time of publication
Tumors develop in liver, lungs, brain, peritoneum and lymph nodes
Hematochezia (passage of fresh blood in stool)
Slow, chronic blood loss
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 25, 2019 on www.thecalgaryguide.com")
Negative-Pressure-Pulmonary-Edema

Incisional-Hernia
 that ↑ risk of infection
Post-op wound Infection
Obesity
Chronic constipation
Chronic cough Pregnancy
↓ clotting factors
Vigorous cough
Severe Hypertension
Seroma
Post-op hematoma Bulging fluid separates High risk
Sutures unsuitable Poor surgical for tension technique
↑ intraabdominal pressure
Fascial Incision separates
Notes:
fascial incision
surgeries* High Risk Surgeries*
Connective tissue disorder
Suboptimal fascial closure
• • •
Emergency surgeries Midline incisions
Acute abdominal surgeries
↓ wound healing/collagen synthesis
Fascial defect at previous incision site
Incisional Hernia:
Protrusion of tissues through prior fascial incision
• Deep wound infection = most common cause of incisional hernias
• Diagnosis on physical exam +/- CT scan if patient is obese
• Treatment = surgery
Bulge at prior incision site
Palpable fascial defect
Bowel and other abdominal contents protrude through defect
Mechanical bowel obstruction (see relevant slide)
Constipation /obstipation
Contents unable to be pushed back through defect (incarceration)
Vascular supply is compromised to herniated contents
Contents become ischemic (strangulated)
Prolonged pressure on skin & bowel over time
Ulceration & ischemia
↓ blood flow to skin layers
Discoloration of skin
Bulge ↑ with coughing/straining
Ulcers extend through bowel wall
Authors: Karly Nikkel Meaghan Ryan Reviewers Michael Blomfield Tony Gu Yan Yu* Edwin Cheng* *MD at time of publication
Colo-enteric fistula
Bowel Perforation
Abdominal Pain
Abdominal Distension
Nausea/ Vomiting
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 13, 2019 on www.thecalgaryguide.com")
Varicocele
.
• Small varicoceles can be identified by preforming the Valsalva maneuver (decreases venous return).
• Unilateral right varicoceles are uncommon and should be investigated for underlying pathology causing obstruction.
Primary
Anatomically: the left spermatic vein drains into the left renal vein
Nutcracker Effect: The left renal vein can get pinched by the abdominal aorta and superior mesenteric artery
Backup of blood in left renal vein ↑ pressure in left spermatic vein
Secondary
Renal cell carcinoma or retroperitoneal masses
Inferior vena cava thrombus
External compression of spermatic vein
Obstruction of blood flow
↑ spermatic vein pressure
Vein valve leaflet failure & retrograde bloodflow back towards testicle
Dilation of pampiniform plexus and scrotal vein plexus
Varicocele
↑ scrotal blood volume ↑ volume in a closed
space
↑ pressure and distension of scrotal layers
↑ scrotal vein plexus pressure
Compliant veins distend, becoming visible through scrotum
Blood heats up the structures it flows through
Scrotal hyperthermia
Unsuitable environment for spermatogenesis
Loss of germ cell mass
Bag of Worms Sign
Dull ache/heaviness
Decreased fertility Testicular atrophy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com")
vomiting-pathogenesis
 Center
Toxins circulating in bloodstream: Chemotherapy, Opioids
Offending substance travels through circulation and binds to receptors in the CTZ, outside the blood brain barrier
Abbreviations:
GERD: Gastroesophageal Reflux Disease PUD: Peptic Ulcer Disease
IBD: Inflammatory Bowel Disease
CTZ: Chemoreceptor Trigger Zone
CNX: Cranial Nerve Ten
H1: Histamine Receptor
M1: Muscarinic Receptor
Disrupted inner ear balance: Motion Sickness
Activation of H1 & M1 receptors in vestibular center traveling via Cerebellum
Stimulates Solitary Tract Nucleus (Medulla)
(Medulla)
Vagus Nerve (CNX) and enteric nervous system activation, resulting in:
Gastric relaxation, ↓ pylorus tone, retrograde duodenal peristalsis
Downward diaphragm contraction, abdominal & chest wall muscles contract: ↑ intra-gastric pressure
Vomiting
(Forceful expulsion of material from stomach and intestines)
Upper and lower esophageal sphincter relaxation and glottis closure
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-published February 16, 2020 on www.thecalgaryguide.com")
Marfan-Syndrome

Dural ectasia
(widening of the dural sac)
Diminished and disorganized dural elastic fibres
Abnormalities in connective tissues
Tear in the aortic intima (innermost layer of aorta)
Aortic dissection
Type A (tear in ascending aorta) > Type B (tear in descending aorta)
Back pain
Sensory and motor deficits
Ectopia lentis
(lens dislocation)
Development of lung bullae and blebs
Rupture of bullae/blebs
Pneumothorax
** Abnormal properties of lens + cornea
** Scoliosis
** Myopia
Tall stature Chest wall (pectus)
Inherited (autosomal dominant) or de novo mutation in FBN1 gene
Distortion of neural roots
Thinning of ciliary zonules of the eye
Weakness and rupture of alveolar tissue
Production of aberrant or reduced fibrillin-1
Formation of unstable microfibrils in extracellular matrix of connective tissues
**
inactivate TGF-β1
↑ production of matrix metalloproteinases
↑ cellular signaling cascades
↑ production of growth factors in the endocardium
Cell proliferation and apoptosis suppression in mitral valve leaflets
Change in valvular architecture
Mitral prolapse
Mitral regurgitation
↑ degradation of extracellular matrix
Thinning of the aortic media
Weakness of the aortic wall
Inability of fibrillin- 1 to sequester and
↑ TGF-β1 signalling
Abbreviations
• TGF-β: Transforming
growth factor beta (a cytokine)
Notes
**The underlying
mechanisms are unclear
Authors:
Tony Gu Reviewers: Amanda Nguyen Davis Maclean Yan Yu* Michelle Keir*
* MD at time of publication
Aortic root dilation
Aortic valve leaflets stretched outwards, unable to fully close
Aortic regurgitation
Aneurysmal dilation of the abdominal & thoracic aorta
Aortic rupture
Stroke
Blood enters and pressurizes a ‘false lumen’
Obstruction of aortic branches
End organ malperfusion
** deformities
** Joint hypermobility
Thumb sign: Thumb tip extends from palm of hand when thumb is folded into closed wrist
Wrist sign: thumb and fifth finger of the hand overlap when grasping opposite wrist
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 28, 2020 on www.thecalgaryguide.com")
acute-pancreatitis-complications
:
Interstitial edematous pancreatitis
Local accumulation of fluid in the pancreas
<2 weeks after onset
Acute peripancreatic fluid collection (not encapsulated)
Walled off by fibrous & granulation tissue
>2 weeks after onset
Pancreatic pseudocyst
(completely encapsulated)
Peritoneal irritation à pain
Large cyst can (very rarely) compress surrounding bowel
Acute Pancreatitis
Inflammatory cytokines are released from damaged pancreas
If recurrentàchronic pancreatitis (see relevant slide)
Inflammation damages pancreatic exocrine
cellsàInappropriate release of pancreatic enzymes into surrounding tissue & vasculature àdigesting pancreatic parenchyma
Authors: Nissi Wei, *Yan Yu Reviewers: Dean Percy, Miles Mannas, Varun Suresh, Brandon Hisey, *Kerri Novak, *Sylvain Coderre * MD at time of publication
complete resolution (most cases)
Necrotic tissue is vulnerable to
infection (esp. Gram neg GI bacteria)
inflammation & necrosis activate cytokine cascade
Severe, necrosis (15%): Necrotizing pancreatitis
Local infection
Severe pancreatic inflammation shifts body fluid into retroperitoneal spaceàintravascular volume depletion
Systemic Inflammatory Response Syndrome (SIRS) (see relevant slide)
Organ failure (may be sole feature on presentation)
Stagnant fluid can more easily become infected
Infection spreads to bloodstream
Cardiac failure Hypovolemic shock Renal failure
Local accumulation of fluid & necrosis in the pancreas
< 4 weeks after onset:
Acute necrotic collection (not encapsulated)
Walled off by fibrous & granulation tissue
> 4 weeks after onset
walled-off necrosis
(completely encapsulated)
When treated with excess fluid resuscitation:
Intra- abdominal hypertension
Respiratory failure (ARDS)
Disseminated intravascular coagulation (DIC)
Bowel obstruction Gastric outlet (see relevant slide) obstruction
Infected pancreatic necrosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 20, 2016, updated September 7, 2020 on www.thecalgaryguide.com")
Pulmonary Hypertension

↓ contractility and/or diastolic relaxation
↓ left ventricle cardiac output Backup of blood in left ventricle and atrium Backup of blood in pulmonary vasculature
↑ pulmonary capillary wedge pressure– estimate of blood pressure in left atrium
Chronic Anemia
↓ plasma hemoglobin content
↓ oxygen carrying capacity per unit blood
Compensatory ↑ in heart rate to maintain tissue oxygen supply
↑ cardiac output
Lung disease (chronic obstructive pulmonary disease)
Tissue breakdown and ↓ lung elasticity
Chronic thromboembolism
Pulmonary vessel disease (pulmonary arterial hypertension, scleroderma)
Vascular obstruction/fibrosis
↓ lungs’ ventilation ability
↓ surface areaà↓ gas exchange
Lung vasculature undergo reflexive, localized vaso- constriction, to shunt blood to better ventilated areas
Chronic hypoxemia
↓ local alveolar partial pressure of oxygen
↓ blood vessel compliance
↑ Pulmonary vascular resistance (PVR)
Impaired gas exchange across thickened vessel walls
↓ blood partial pressure of O2 and ↑ partial pressure of CO2
Insufficient O2 provision & CO2 removal from tissues
Reflexive mechanisms trigger harder & faster breathing to compensate
Vascular fibrosis due to chronically increased pressures
↓ circulation of blood to left heart and ↓ filling of left ventricle
↓ left ventricle cardiac output
Elevated blood pressure in the lung arteries Pulmonary Hypertension
↑ right-ventricle afterload (pressure against which the heart contracts to eject blood)
↓ right ventricle cardiac output
↑ residual volume in right heart after cardiac contraction
Backup of blood in systemic circulation ↑ blood volume in venous system
Myocardial hypertrophy develops over time (eccentric & concentric)
↑ tissue volume
↑ myocardial oxygen demand
Myocardial ischemia (supply/demand mismatch)
↑ risk of chest pain in times of ↑ oxygen demand
Peripheral edema
Formation of aberrant conduction pathways and ectopic electrical foci
Dysrhythmias
Palpitations
↓ tissue perfusion
Fatigue
Dyspnea
↓ brain perfusion
Syncope
Authors: Grant E. MacKinnon Davis Maclean Hannah Yaphe Reviewers: Yan Yu* Jason Weatherald* * MD at time of publication
↑ volume and blood pressure in capillaries Fluid pushed from vessels into interstitial space of tissues
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 8, 2020 on www.thecalgaryguide.com")
Tumour-Lysis-Syndrome

Though rare, aggressive tumours can spontaneously lyse without treatment
Intracellular potassium released into bloodstream
Intracellular phosphate released
Hyperphosphatemia
↑ serum phosphate
Intracellular lactate dehydrogenase (LDH) released
↑ serum LDH
Intracellular nucleic acids released
Nucleic acids metabolized to uric acid
Hyperuricemia
↑ serum uric acid
Hyperkalemia
↑ serum potassium
(see Hyperkalemia: clinical findings)
Uric acid (a crystallizing substance) ↑ precipitation of calcium phosphate
↑ filtration of poorly soluble uric acid into acidic environment of renal tubules
Serum phosphate binds serum calcium, forming solid calcium phosphate precipitate crystals
High levels of calcium phosphate ↑ uric acid precipitation
Uric acid precipitates as crystals and deposits in kidney tubules and collecting ducts
Tubular injury and/or intraluminal obstruction
Endothelial dysfunction in renal vasculature
Renal inflammation, vasoconstriction, and
impaired renal vascular autoregulation
Decreased renal filtration
Acute Kidney Injury
(see Acute Kidney Injury Overview)
Crystal deposition in the heart
Depletion of soluble calcium
Hypocalcemia
Calcium phosphate crystals deposit in kidneys
Main mechanism of Acute Kidney Injury
Cardiac Arrythmias
↓ serum calcium
(see Hypocalcemia: clinical findings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 25, 2020 on www.thecalgaryguide.com")
Small-Bowel-Obstruction-findings-on-X-Ray
 proximal to the obstruction
Gas rises above the fluid
If exclusively or mostly accumulation of fluid (and not gas) occurs
Any small amounts of gas/air present (not enough to create an
air-fluid level) will rise and become trapped in valvulae conniventes (small bowel folds)
Small bowel loops are anatomically
central compared to large bowel
Bowel contents physically push on the bowel walls, dilating them
Dilated bowel loops are “central” in location on the x-ray
Dilated bowel loops (>3cm)
Valvulae Conniventes Visible: Anatomical folds of the small bowel that becomes more
apparent when small bowel is distended & allows differentiation from large bowel
Air-fluid level (on erect/upright study)
- Dark area above level = Gas/Air
- Bright/white area below level = Fluid
‘Gasless’ abdomen (not seen here): Refers to the lack of gas/air (dark on X-ray) in the bowel loops - only fluid (bright/white on X- ray) is seen in bowel loops
String of pearls sign (not seen here):
Small gas bubbles seen arranged in a “string of pearls” pattern instead of a large air fluid level
Image Credit: Alberta Health Services Repository
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 25, 2020 on www.thecalgaryguide.com")
Fat-Embolism-Syndrome

Non-trauma related (rare)
Long bone fracture
Pelvic fracture
Orthopedic Trauma
Intraosseous access
Soft tissue injuries
Chest compressions
Bone marrow transplant
Pancreatitis
Diabetes mellitus
Fat from bone marrow is disrupted and leaks into bloodstream via damaged blood vessels
Fat globules obstruct dermal capillaries
Capillaries rupture
Blood leaks into the skin
Petechial rash
Non-Orthopedic Trauma (less common)
Fat from injured adipose tissue is released from adipocytes into bloodstream
Metabolic disturbance mobilizes stored fat and moves it into circulation
Fat Embolism Syndrome
the presence of fat globules in circulation
Fat globules damage blood vessel walls
Platelets stick to damaged areas Platelet aggregation
↑ circulating free fatty acids
↑ inflammatory cytokines (TNF, IL1, IL6)
↑ serum C Reactive Protein (an acute phase reactant)
C reactive protein binds to lipid vesicles in circulation
↑ formation of lipid complexes in the blood
Obstruction of cerebral vasculature
↓ blood flow and oxygen delivery to brain tissue
Neurological findings: ranging from ↓ level of consciousness to seizures
Notes:
Large quantities of fat globules can obstruct pulmonary vasculature
Blood clots form throughout the body
Disseminated intravascular coagulopathy
Back up of blood into right heart àRight ventricular dysfunction
↓ pulmonary arterial blood flow à↓ gas exchange in the lungs
Higher CO2 & lower O2 levels in blood àdetected by chemoreceptors
Chemoreceptors stimulate respiratory centre in the brain to ↑ rate of respiration
Dyspnea / Tachypnea
Authors: Tabitha Hawes Reviewers: Hannah Koury, Alyssa Federico, Davis MacLean, Mehul Gupta, Yan Yu*, Jeremy Lamothe* * MD at time of publication
• Underlined findings indicate classic triad of symptoms (petechial rash, neurologic findings, dyspnea/tachypnea)
• Clinical presentation of fat embolism syndrome is variable and may present with any or all of these findings
↓ pumping of blood into systemic circulation
Hypotension Obstructive shock
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 19, 2021 on www.thecalgaryguide.com")
Complications-Accouchement-Vaginale
 et la cicatrisation des vaisseaux, le tissu cicatriciel est éliminé de l'utérus.
Lochies (pertes/ saignements vaginaux) et perte d'escarres (tissu cicatriciel)
Le tissu placentaire peut être retenu dans l'utérus.
L'utérus ne se
contracte pas complètement pour fermer les vaisseaux sanguins utérins.
Hémorragie post- partum (Voir la diapositive correspondante)
Les substances étrangères déclenchent une réaction inflammatoire systémique chez la mère
Coagulation intravasculaire disséminée, CIVD (voir diapositive correspondante)
Dans de rares cas, des vaisseaux sanguins déchirés laissent le liquide amniotique (contenant des cellules fœtales et du méconium) pénétrer dans la circulation maternelle.
Embolie de liquide amniotique (amas de cellules fœtales et de méconium dans la circulation maternelle)
Le liquide amniotique visqueux peut bloquer les vaisseaux sanguins maternels
Obstruction de la circulation du sang dans les poumons
Bas debit cardiaque avec reduction de la précharge.
Tissus endommagés et sang dans l'utérus
Des nutriments pour que les bactéries infectent l'utérus.
Endométrite
Douleur
utérine, irradiant dans tout l'abdomen
Œdème pulmonaire
Hypotension
Manque de perfusion au cœur Arrêt cardiaque
Le passage du fœtus distend les muscles pubo- vésiculaires et pubo-rectaux.
L'urètre/ rectum ne sont plus suffisamment courbés pour empêcher les fortes pressions intra- abdominales de forcer l'urine ou les selles.
Incontinence de stresse
(de la vessie et des intestins ; généralement temporaire)
Remarque: la dépression post-partum est couramment observée chez au moins 10 % des mères qui viennent d'accoucher.
Déchirures
périnéales (1er-4e degré) ; Hémorroïdes
Douleur périnéale
Douleur et gonflement
unilatéral de la jambe
Dyspnée, Toux
Les lésions tissulaires activent les facteurs de coagulation du sang.
Coagulation
dans les zones d'hémostase (par exemple, les veines)
Thrombose veineuse profonde
La fièvre du post- partum
(voir la diapositive correspondante)
L'insertion d'un tube étranger dans la vessie facilite la colonisation de la vessie et des voies urinaires par les bactéries.
Infections des voies urinaires
Si grave
Effondrement cardio-vasculaire
Légende:
Pathophysiologie
Méchanisme
Signe/Symptôme/Résultat Laboratoire
Complications
Publié 19 juin 2013 à www.thecalgaryguide.com")
cystic-fibrosis-findings-on-chest-x-ray-and-lung-window-ct-scan
, Mark Montgomery* * MD at time of publication
Collapsed alveoli appears white on x-ray
Peribronchial Cuffing
secretions become more viscous. (See relevant slide for CF pathogenesis.)
As early as at birth, secretions collect in bronchial lumen, delaying mucociliary clearance
Mucus plugs and obstructs bronchial lumen
Air trapped distal to obstruction and cannot leave lungs
Lung Hyperinflation
Diaphragm domes below 10th posterior rib and 6th anterior rib on PA CXR
Flattened hemidiaphragm, enlarged retrosternal space on lateral CXR
With time, pulmonary capillaries gradually absorb gases in alveoli distal to obstruction àalveolar collapse (Atelectasis)
Collapsed alveoli more solid and radiodense than airà↓X-ray penetration
Adjacent structures may shift towards atelectasis on CXR
In first few years of life, retained bronchial secretions serve as nidus for recurrent bacterial colonization and infection
Late findings at 10- 30 years oldà secretion accumulation blocks inhaled air to affected lung segments àchronic hypoxia
Inflammatory response (cytokines, nitric oxide and radical oxygen species) leads to bronchial and peribronchial destruction
Hypoxia induces pulmonary capillary vasoconstriction
Some airways are blocked more than others
Leakage of fluid into bronchial walls & peri- bronchial regions.
Inflammatory cytokines destroy elastic components of bronchi
Accumulation of inflammatory exudate in bronchi
Pulmonary artery hypertension à Blood backs up in pulmonary arteries
Some segments of lung underventilated
Fluid around bronchial walls is more radiodense than air à↓X-ray penetration àappears white
Bronchiectasis: dilated, thickened, untapered bronchi on CXR/CT
Fluid/mucus in bronchi is more radiodense than air, thus appearing white on imaging
Edematous bronchi viewed end on are thickened and appear ring-like on CT/CXR
Tramlines (AKA Tramtracking)
Bronchus wider than corresponding blood vessel on CXR/CT
Advanced bronchiectasis is saccular in appearance
Mucus-filled bronchi form tubular opacities giving appearance of white fingers on CXR/CT
Signet Ring Sign
Bronchiectatic Cavities
Mucoid Impaction (AKA Finger in glove sign)
↑ Blood dilates pulmonary arteries
Blood backs up in right ventricle, dilating it
Pulmonary arteries look wider on CXR.
Main pulmonary artery >30 mm diameter on CT
Right Ventricle Enlargement on CXR/CT
Underventilated lung segments appear as lower intensity (darker) than normal ventilated segments which appear as normal intensity (brighter)
Mosaic Changes on CT(non- contrast
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 13, 2013, updated Aug 18, 2021 on www.thecalgaryguide.com")
asthma-pathogenesis
 Naushad Hirani* * MD at time of publication
Genetic factors
(i.e. HLA gene mutations, defects in bronchial airway epithelium)
Environmental factors
(i.e. excess hygiene, fewer siblings, antibiotics within the first two years)
Asthma:
Defined as airway hyper-responsiveness causing variable and reversible airflow obstruction
Atopy:
predisposition to allergic hyper-sensitivity in airways
First exposure to triggers*
sensitizes helper T cells
Stimulation of B-cells to produce IgE, which binds to mast cell surfaces
Activated Helper-T cells & IgE-sensitized mast cells now line the airways
Triggers of airway hyper- responsiveness include:
Upper respiratory tract infections (URTIs)
Allergens (pollen, animal dander, dust, mold, etc)
Air pollution, cigarette smoke, other chemicals
Drugs (aspirin, NSAIDs, Beta- blockers)
Cold air
Exercise
Early response (0-2 hrs)
Delayed response (3-4 hrs)
Allergens cross-link IgEs on mast cells
Activated mast cells & helper T cells release cytokines
Mast cells release histamines, leukotrienes, and other inflammatory mediators
Induce maturation of granular WBCs like eosinophils
Eosinophils migrate into:
Vascular permeabilityà edema of airway mucosa
Goblet cell hyperplasia à mucus secretion
Bronchial smooth muscle contraction
Airway obstruction
Second exposure to triggers
Asthma Airways Bronchiole constriction
Eyes Conjunctivitis Nose Rhinitis
Note: Delayed response presents within 3-4 hrs, peaks within 6-8 hrs, and resolves within 24 hrs
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 17, 2012, updated Aug 19, 2021 on www.thecalgaryguide.com")
copd-overview-and-definitions
”
Author: Yan Yu Reviewers: Jason Baserman, Jennifer Au, Ciara Hanly, Zesheng Ye (叶泽生), Yonglin Mai (麦泳琳)*, Naushad Hirani*, Juri Janovcik* * MD at time of publication
Cystic Fibrosis
Multisystem disease due to CFTR gene mutation, that presents in the lungs as bronchiectasis
Bronchiectasis, Cystic Fibrosis, etc
COPD
Systemic disease, largely manifesting as an airflow-obstructing respiratory disorder; can manifest in the form of any of the following disorders:
Emphysema
Lung tissue destruction & abnormal, permanent enlargement of lung acini: airspaces distal to terminal bronchioles
Chronic Bronchitis
Chronic, productive cough for a total duration of 3 months per year, over 2 continuous years
Asthma
Asthma that does not
remit completely with treatment (thus, chronic airflow obstruction) is defined as asthma-COPD overlap syndrome (ACOS)
Emphysema
Bronchiectasis
Destruction and widening of large airways, resulting in mucus hyper-secretion and recurrent infections
Chronic Bronchitis
Most common COPD manifestations
(most patients suffer from a combination of emphysema and chronic bronchitis)
Clinically, COPD is seen as:
• Progressive, partially reversible airflow obstruction and lung hyperinflation (causing respiratory symptoms like cough, sputum production, and dyspnea)
• Post-bronchodilator spirometry results: FEV1/FVC ratio <0.7 (FEV1 is not a defining feature of COPD, but a marker of severity)
• ↑ frequency & severity of acute exacerbations
• Systemic manifestations such as
deconditioning and muscle weakness
Chronic Obstructive Pulmonary Disease (COPD)
Asthma
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013, updated October 5, 2021 on www.thecalgaryguide.com")
Ectopic Pregnancy

Endometriosis
Tubal surgery or disorders
Age >35
Risk factor accumulation over time
Smoking
Impairment in tubal motility; impaired immunity (risk factor for PID)
Tubal scarring leading to adhesions, obstruction, and alteration of tubal function
Ectopic Pregnancy:
Implantation of developing blastocyst outside the uterine cavity, most commonly in fallopian tube (other locations: interstitial > cornual > cervical > ovarian > abdominal)
Embryo releases human chorionic gonadotropin (β-hCG), which supports corpus luteum to continue producing progesterone
On transvaginal ultrasound: Extrauterine gestational sac with a yolk sac or embryo
Embryo & trophoblast deathàloss of hormone support for the decidua (modified endometrial lining)
Progesterone maintains the endometrial lining, preventing it from shedding
Missed period
Penetration of ovum into muscular wall of fallopian tube
Tubal distention àTubal rupture
Intra-abdominal hemorrhage
Pregnancy cannot survive without the uterine endometrium
Maternal blood extrudes through fimbriae of fallopian tubes and into peritoneal cavity
Lower abdominal pain (including peritonitis in cases of hemoperitoneum)
Hemoperitoneum
(blood in the peritoneal cavity)
Sloughing of decidua out of the uterus through the vagina
Vaginal bleeding (usually in first trimester)
Cessation of human chorionic gonadotropin (β-hCG) release from embryo
β-hCG plateaus or decreases
Authors: Jemimah Raffé-Devine Tahsin Khan Yan Yu* Reviewers: Brianna Ghali Bishwas Paudel Mackenzie Grisdale Christina Schweitzer Ron Cusano* Jadine Paw* * MD at time of publication
Syncope
↓ Level of consciousness
Positive β-hCG, but rising <35% over 2 days
Discriminatory zone: β-hCG >2000 + absence of intrauterine pregnancy
Hypotension
Shock
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 1, 2017, updated Oct 19, 2021 on www.thecalgaryguide.com")
Summary of Cyanotic Congenital Heart Diseases

Authors: Winnie Nagesh, Gaya Narendran, Deborah Fruitman* Reviewers: Austin Laing, Yan Yu* * MD at time of publication
Right heart normally carries deoxygenated blood to the pulmonary circulation while the left heart carries oxygenated blood to the systemic circulation.
Cyanosis can be due to varied pathophysiology, most involve a R-L shunt (described below)
Typically presents in the newborn period but depends on the severity and the type of lesion
Tetralogy Of Fallot (TOF)
Main features: 1.VSD, 2. Overriding aorta, 3. RVH, 4. Pulmonary Valve stenosis
1. VSD causes equal systolic pressure in R and L ventricles
2. Pulmonary Valve stenosisàRight Ventricle Outflow
Tract Obstructionà↓ pulmonary blood flow (degree
depends on severity of obstruction)
3. RVàLV flow across VSD
Presents in the 1st days to weeks, depending on severity of pulmonary valve stenosis
On exam: LUSB SEM; loud S2; hypoxemia (degree depends on severity of Right Ventricle Outflow Tract Obstruction)
CXR: “boot-shaped” heart, decreased pulmonary vasculature
Presents at birth
On exam: Often no murmur, no respiratory distress, severe cyanosis/hypoxemia
CXR: “egg on a string”, normal pulmonary vasculature
Presents in the 1st days to weeks as CHF symptoms develop On exam: Systolic ejection click, Single S2 , SEM, mild hypoxemia due to mixing of blood, +/- tachypnea, hepatomegaly (CHF symptoms)
CXR: normal or ↑ pulmonary vasculature
Presentation varies based on the degree of the outflow tract obstruction
On exam: +/- Holosystolic murmur at LLSB (from VSD), or SEM if outflow tract obstruction, +/- severe cyanosis dependent on severity of pulmonary stenosis
CXR: normal or ↓ pulmonary vasculature
Presents in early infancy (earlier and more severe presentation if obstructed)
On exam: +/-split S2, SEM LUSB, tachypnea, mild cyanosis CXR: cardiomegaly with ↑ pulmonary vasculature
Note: see relevant Calgary Guide slides for each heart condition for full explanation of their pathophysiology. Figures are hand-drawn by the authors.
Transposition of the Great Arteries (TGA)
Aorta is the outflow for RV and pulmonary artery is the outflow for the LV (parallel circulation)
Truncus Arteriosus
1. Single vessel (truncus) fails to divide into pulmonary artery and aorta, 2. Single outlet overriding VSD
Tricuspid Atresia
Tricuspid valve fails to develop normally with a
hypoplastic right heart and VSD
1. Deoxygenated blood pumped from RVàaortaà systemic circulation, bypassing the lungs.
2. Oxygenated blood pumped from LVàPA
1. RV + LV pumped through VSDàoverriding truncal artery 2. Mixed deoxygenated and oxygenated blood enters
systemic, pulmonary and coronary circulations
1. Blood cannot enter RV due to lack of tricuspid valve
2. Deoxygenated blood pumped from RAàASDàLA and
mixes with oxygenated blood
3. Mixed blood enters systemic circulation
Total Anomalous Pulmonary Venous Return (TAPVR)
Pulmonary veins return blood to systemic venous circulation (most common type of supracardiac congential heart disease)
1. Oxygenated blood flows through pulmonary veinsàenters Superior or Inferior Vena CavaàRight atrium (all systemic & pulmonary venous blood returns to the RA, resulting in mixing of blood)
2. Blood follows pressure gradient, flows from RAàLA via ASD
3. Flow from LAàLVàAortaàSystemic Circulation
Abbreviations: VSD: Ventral Septal Defect; RVH: Right Ventricular Hypertrophy; RV: Right Ventricle, LLSB: Left Lower Sternal Border, LUSB: Left Upper Sternal Border; SEM: Systolic ejection Murmur; RVOTO: Right Ventricle Outflow Tract Obstruction
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 21, 2021 on www.thecalgaryguide.com")
COPD-发病机制
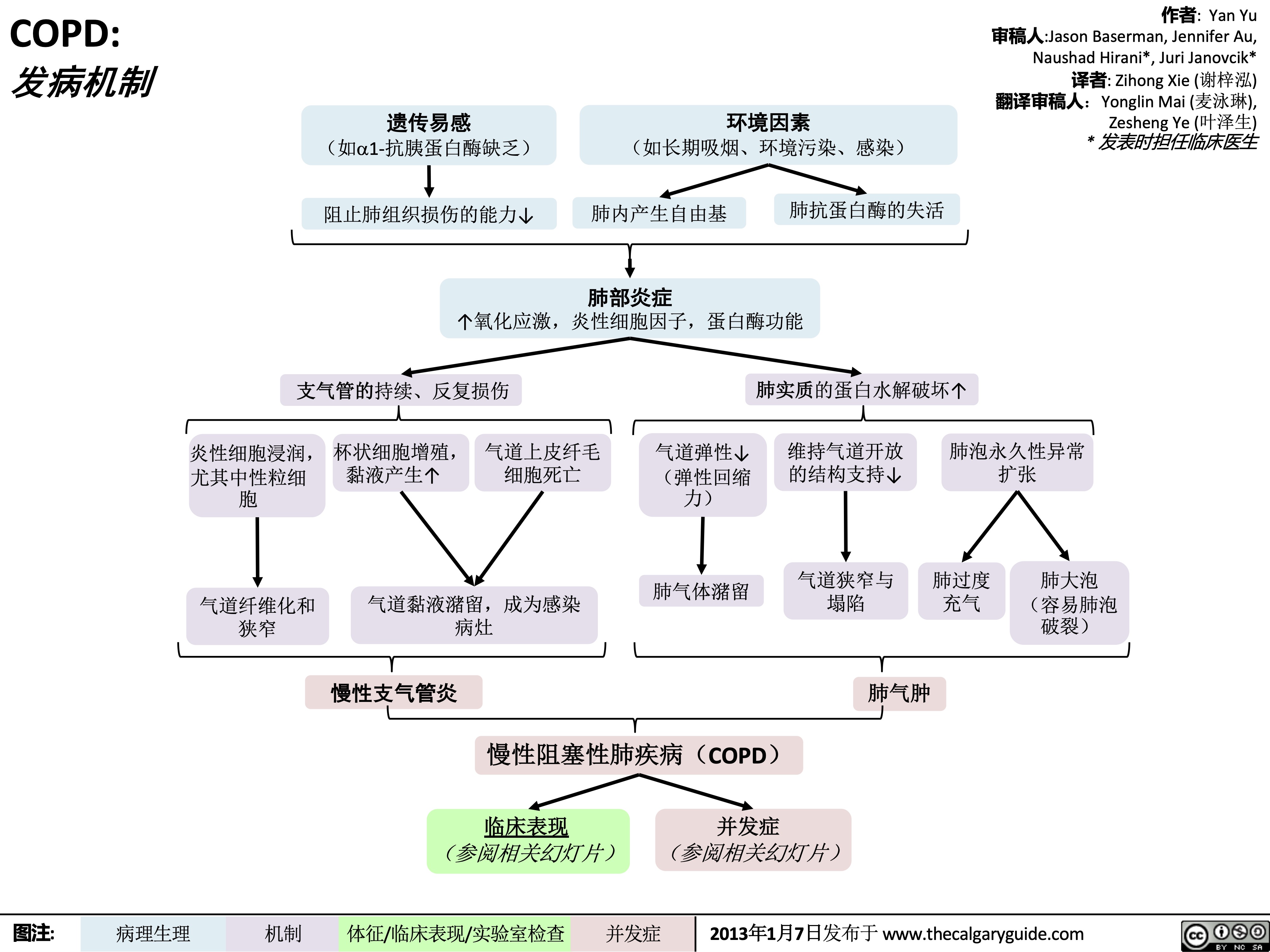 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" title="COPD: 发病机制
作者: Yan Yu 审稿人:Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人:Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
/012
(如a1-抗胰蛋白酶缺乏) 阻止肺组织损伤的能力↓
+,-.
(如长期吸烟、环境污染、感染)
肺内产生自由基
34*5
肺抗蛋白酶的失活
↑氧化应激,炎性细胞因子,蛋白酶功能
支气管的持续、反复损伤
炎性细胞浸润, 杯状细胞增殖, 气道上皮纤毛 尤其中性粒细 黏液产生↑ 细胞死亡
气道弹性↓ (弹性回缩
肺实质的蛋白水解破坏↑ 维持气道开放 肺泡永久性异常
的结构支持↓ 扩张
胞 力)
肺气体潴留 气道狭窄与 肺过度 肺大泡
气道黏液潴留,成为感染 狭窄 病灶
塌陷 充气
肺气肿
(容易肺泡 破裂)
气道纤维化和
%&'()*
慢性阻塞性肺疾病(COPD)
临床表现 并发症 (参阅相关幻灯片) (参阅相关幻灯片)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Clinical Findings Lung tissue
Chronic Obstructive Pulmonary Disease (COPD)
damage
↓ elastic recoil to push air out of lungs on expiration
Lungs don’t fully empty, air is trapped in alveoli (lung hyperinflation)
↑ lung volume means diaphragm is tonically contracted (flatter)
If occurring around airways
Airflow obstruction
↑ mucus production
↓ number of epithelial ciliated cells to clear away the mucus (the cells have been killed by airway inflammation)
Chronic cough with sputum
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
↓ perfusion of body tissues (i.e. brain, muscle)
Fatigue; ↓ exercise tolerance
Total expiration time takes longer than normal
Prolonged expiration
More effort needed to ventilate larger lungs
Respiratory muscles must work harder to breathe
Turbulent airflow in narrower airways is heard on auscultation
Expiratory Wheeze
Diaphragm can’t flatten much further to generate deep breaths
To breathe, chest wall must expand out more
Dyspnea
Shortness of breath, especially on exertion
Breathes are rapid & shallow
If end-stage:
Chronic fatigue causes deconditioning
Muscle weakness & wasting
Barrel chest
If end-stage: diaphragm will be “flat”. Continued
Patient tries to expire against higher mouth air pressure, forcing airways to open wider
Pursed-lip breathing
Patient breathes with accessory muscles as well as diaphragm to try to improve airflow
inspiratory effort further contracts diaphragmà pull the lower chest wall inwards
Hoover’s sign
(paradoxical shrinking of lower chest during inspiration)
Tripod sitting position (activates pectoral muscles)
Neck (SCM, scalene) muscles contracted
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$
慢性阻塞性肺疾病 (COPD) 如果出现在气道周围 气流阻塞
肺不能完全排空
气体,气体潴留
于肺泡(肺过度
充气)
总呼气时长大于 正常时长
呼气相延长
肺组织损伤
呼气时,将空气排出肺外 的弹性回缩力↓
肺不能完全排空气体,
气体潴留于肺泡内
(肺过度充气)
肺容积↑,膈肌紧张 性收缩(膈肌平坦)
呼气时,胸膜腔正压挤压气道 à 气道阻塞↑
肺泡通气↓ 血液氧合↓ (低
氧血症)
身体组织灌注 量↓ (比如脑、 肌肉)
疲劳; 运动耐量↓
黏液生成↑ 清除黏液的上皮纤
毛细胞数量↓ (受 气道炎症损伤)
慢性咳嗽伴咳 痰
作者: Yan Yu
审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳),
Zesheng Ye (叶泽生)
* 发表时担任临床医生
容积较大 的肺需要
更加努力 才能通气
呼吸肌必须
更用力才能 呼吸
听诊闻及狭窄气
道中的湍流气流
呼气喘鸣音
呼吸困难 气促,尤其是劳累
膈肌无法进一步收缩以
产生深呼吸
呼吸浅快
为了呼吸,
胸壁必须延
展得更大
桶状胸
晚期病人:
患者试图在较高的口 慢性疲劳导致 患者动用辅助呼吸肌和膈肌呼吸,
腔内气压下进行呼气, 活动耐量下降 从而使气道更开放
以改善气流
晚期病人:膈肌 “平坦” ,持续吸气进一步压 缩膈肌à 向内拉季肋部胸壁
胡佛征 (吸气时,胸廓下侧季肋部内收)
缩唇呼吸
肌肉无力 & 消瘦
端坐呼吸 (调动胸肌)
颈部肌肉收
缩(胸锁乳
突肌、斜角
肌)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Findings on Investigations
Chronic Obstructive Pulmonary Disease (COPD)
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
Airflow obstruction
Lung tissue damage
↓ ventilation of alveoli
Blood perfusing ill- ventilated alveoli does not receive normal amounts of oxygen
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction)
No elastic recoil to push air out of lungs
Loss of lung parenchyma and vasculature ↓ surface area for gas exchange
↓ diffusion capacity
(on spirometry)
Hypoxemia: PaO2 < 70mmHg (on ABGs)
Abbreviations:
• FEV1: Forced expiratory volume in 1 second
• FVC: Forced vital capacity
• TLC: Total lung capacity
• VC: Vital Capacity
Investigations for COPD :
• Spirometry (Pulmonary function test)
Total expiration time takes longer than normal
FEV1/FEV < 0.7
(on spirometry)
Lungs don’t fully empty
More air trapped within lungs (hyperinflation)
More CO2 remains and diffuses into the blood
Hypercapnia: PaCO2 > 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" />
45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" title="COPD: 发病机制
作者: Yan Yu 审稿人:Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人:Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
/012
(如a1-抗胰蛋白酶缺乏) 阻止肺组织损伤的能力↓
+,-.
(如长期吸烟、环境污染、感染)
肺内产生自由基
34*5
肺抗蛋白酶的失活
↑氧化应激,炎性细胞因子,蛋白酶功能
支气管的持续、反复损伤
炎性细胞浸润, 杯状细胞增殖, 气道上皮纤毛 尤其中性粒细 黏液产生↑ 细胞死亡
气道弹性↓ (弹性回缩
肺实质的蛋白水解破坏↑ 维持气道开放 肺泡永久性异常
的结构支持↓ 扩张
胞 力)
肺气体潴留 气道狭窄与 肺过度 肺大泡
气道黏液潴留,成为感染 狭窄 病灶
塌陷 充气
肺气肿
(容易肺泡 破裂)
气道纤维化和
%&'()*
慢性阻塞性肺疾病(COPD)
临床表现 并发症 (参阅相关幻灯片) (参阅相关幻灯片)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Clinical Findings Lung tissue
Chronic Obstructive Pulmonary Disease (COPD)
damage
↓ elastic recoil to push air out of lungs on expiration
Lungs don’t fully empty, air is trapped in alveoli (lung hyperinflation)
↑ lung volume means diaphragm is tonically contracted (flatter)
If occurring around airways
Airflow obstruction
↑ mucus production
↓ number of epithelial ciliated cells to clear away the mucus (the cells have been killed by airway inflammation)
Chronic cough with sputum
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
↓ perfusion of body tissues (i.e. brain, muscle)
Fatigue; ↓ exercise tolerance
Total expiration time takes longer than normal
Prolonged expiration
More effort needed to ventilate larger lungs
Respiratory muscles must work harder to breathe
Turbulent airflow in narrower airways is heard on auscultation
Expiratory Wheeze
Diaphragm can’t flatten much further to generate deep breaths
To breathe, chest wall must expand out more
Dyspnea
Shortness of breath, especially on exertion
Breathes are rapid & shallow
If end-stage:
Chronic fatigue causes deconditioning
Muscle weakness & wasting
Barrel chest
If end-stage: diaphragm will be “flat”. Continued
Patient tries to expire against higher mouth air pressure, forcing airways to open wider
Pursed-lip breathing
Patient breathes with accessory muscles as well as diaphragm to try to improve airflow
inspiratory effort further contracts diaphragmà pull the lower chest wall inwards
Hoover’s sign
(paradoxical shrinking of lower chest during inspiration)
Tripod sitting position (activates pectoral muscles)
Neck (SCM, scalene) muscles contracted
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$
慢性阻塞性肺疾病 (COPD) 如果出现在气道周围 气流阻塞
肺不能完全排空
气体,气体潴留
于肺泡(肺过度
充气)
总呼气时长大于 正常时长
呼气相延长
肺组织损伤
呼气时,将空气排出肺外 的弹性回缩力↓
肺不能完全排空气体,
气体潴留于肺泡内
(肺过度充气)
肺容积↑,膈肌紧张 性收缩(膈肌平坦)
呼气时,胸膜腔正压挤压气道 à 气道阻塞↑
肺泡通气↓ 血液氧合↓ (低
氧血症)
身体组织灌注 量↓ (比如脑、 肌肉)
疲劳; 运动耐量↓
黏液生成↑ 清除黏液的上皮纤
毛细胞数量↓ (受 气道炎症损伤)
慢性咳嗽伴咳 痰
作者: Yan Yu
审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳),
Zesheng Ye (叶泽生)
* 发表时担任临床医生
容积较大 的肺需要
更加努力 才能通气
呼吸肌必须
更用力才能 呼吸
听诊闻及狭窄气
道中的湍流气流
呼气喘鸣音
呼吸困难 气促,尤其是劳累
膈肌无法进一步收缩以
产生深呼吸
呼吸浅快
为了呼吸,
胸壁必须延
展得更大
桶状胸
晚期病人:
患者试图在较高的口 慢性疲劳导致 患者动用辅助呼吸肌和膈肌呼吸,
腔内气压下进行呼气, 活动耐量下降 从而使气道更开放
以改善气流
晚期病人:膈肌 “平坦” ,持续吸气进一步压 缩膈肌à 向内拉季肋部胸壁
胡佛征 (吸气时,胸廓下侧季肋部内收)
缩唇呼吸
肌肉无力 & 消瘦
端坐呼吸 (调动胸肌)
颈部肌肉收
缩(胸锁乳
突肌、斜角
肌)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Findings on Investigations
Chronic Obstructive Pulmonary Disease (COPD)
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
Airflow obstruction
Lung tissue damage
↓ ventilation of alveoli
Blood perfusing ill- ventilated alveoli does not receive normal amounts of oxygen
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction)
No elastic recoil to push air out of lungs
Loss of lung parenchyma and vasculature ↓ surface area for gas exchange
↓ diffusion capacity
(on spirometry)
Hypoxemia: PaO2 < 70mmHg (on ABGs)
Abbreviations:
• FEV1: Forced expiratory volume in 1 second
• FVC: Forced vital capacity
• TLC: Total lung capacity
• VC: Vital Capacity
Investigations for COPD :
• Spirometry (Pulmonary function test)
Total expiration time takes longer than normal
FEV1/FEV < 0.7
(on spirometry)
Lungs don’t fully empty
More air trapped within lungs (hyperinflation)
More CO2 remains and diffuses into the blood
Hypercapnia: PaCO2 > 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" />
COPD-临床表现
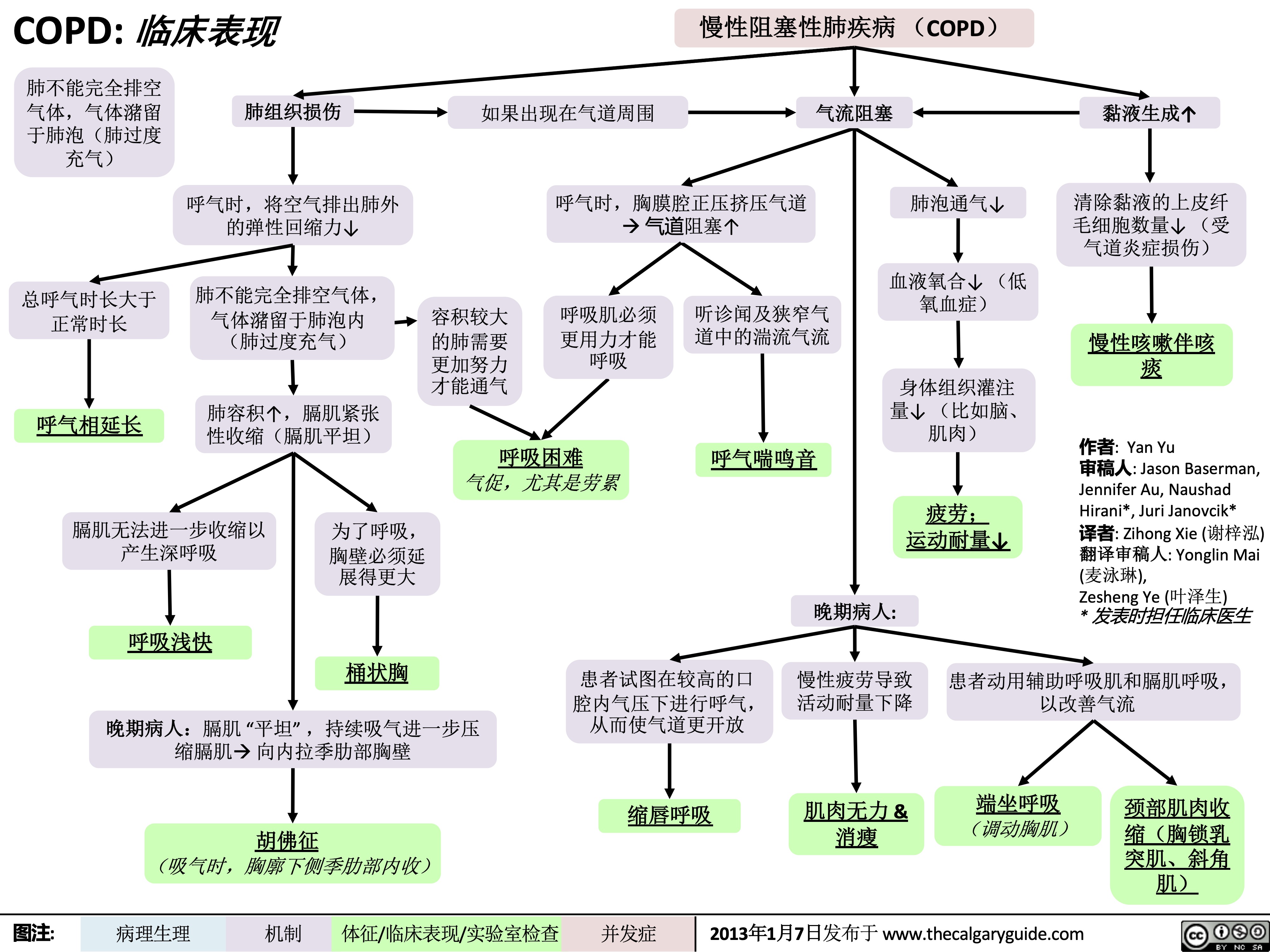 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" title="COPD: 临床表现
作者: Yan Yu 审稿人:Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人:Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
/012
(如a1-抗胰蛋白酶缺乏) 阻止肺组织损伤的能力↓
+,-.
(如长期吸烟、环境污染、感染)
肺内产生自由基
34*5
肺抗蛋白酶的失活
↑氧化应激,炎性细胞因子,蛋白酶功能
支气管的持续、反复损伤
炎性细胞浸润, 杯状细胞增殖, 气道上皮纤毛 尤其中性粒细 黏液产生↑ 细胞死亡
气道弹性↓ (弹性回缩
肺实质的蛋白水解破坏↑ 维持气道开放 肺泡永久性异常
的结构支持↓ 扩张
胞 力)
肺气体潴留 气道狭窄与 肺过度 肺大泡
气道黏液潴留,成为感染 狭窄 病灶
塌陷 充气
肺气肿
(容易肺泡 破裂)
气道纤维化和
%&'()*
慢性阻塞性肺疾病(COPD)
临床表现 并发症 (参阅相关幻灯片) (参阅相关幻灯片)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Clinical Findings Lung tissue
Chronic Obstructive Pulmonary Disease (COPD)
damage
↓ elastic recoil to push air out of lungs on expiration
Lungs don’t fully empty, air is trapped in alveoli (lung hyperinflation)
↑ lung volume means diaphragm is tonically contracted (flatter)
If occurring around airways
Airflow obstruction
↑ mucus production
↓ number of epithelial ciliated cells to clear away the mucus (the cells have been killed by airway inflammation)
Chronic cough with sputum
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
↓ perfusion of body tissues (i.e. brain, muscle)
Fatigue; ↓ exercise tolerance
Total expiration time takes longer than normal
Prolonged expiration
More effort needed to ventilate larger lungs
Respiratory muscles must work harder to breathe
Turbulent airflow in narrower airways is heard on auscultation
Expiratory Wheeze
Diaphragm can’t flatten much further to generate deep breaths
To breathe, chest wall must expand out more
Dyspnea
Shortness of breath, especially on exertion
Breathes are rapid & shallow
If end-stage:
Chronic fatigue causes deconditioning
Muscle weakness & wasting
Barrel chest
If end-stage: diaphragm will be “flat”. Continued
Patient tries to expire against higher mouth air pressure, forcing airways to open wider
Pursed-lip breathing
Patient breathes with accessory muscles as well as diaphragm to try to improve airflow
inspiratory effort further contracts diaphragmà pull the lower chest wall inwards
Hoover’s sign
(paradoxical shrinking of lower chest during inspiration)
Tripod sitting position (activates pectoral muscles)
Neck (SCM, scalene) muscles contracted
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$
慢性阻塞性肺疾病 (COPD) 如果出现在气道周围 气流阻塞
肺不能完全排空
气体,气体潴留
于肺泡(肺过度
充气)
总呼气时长大于 正常时长
呼气相延长
肺组织损伤
呼气时,将空气排出肺外 的弹性回缩力↓
肺不能完全排空气体,
气体潴留于肺泡内
(肺过度充气)
肺容积↑,膈肌紧张 性收缩(膈肌平坦)
呼气时,胸膜腔正压挤压气道 à 气道阻塞↑
肺泡通气↓ 血液氧合↓ (低
氧血症)
身体组织灌注 量↓ (比如脑、 肌肉)
疲劳; 运动耐量↓
黏液生成↑ 清除黏液的上皮纤
毛细胞数量↓ (受 气道炎症损伤)
慢性咳嗽伴咳 痰
作者: Yan Yu
审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳),
Zesheng Ye (叶泽生)
* 发表时担任临床医生
容积较大 的肺需要
更加努力 才能通气
呼吸肌必须
更用力才能 呼吸
听诊闻及狭窄气
道中的湍流气流
呼气喘鸣音
呼吸困难 气促,尤其是劳累
膈肌无法进一步收缩以
产生深呼吸
呼吸浅快
为了呼吸,
胸壁必须延
展得更大
桶状胸
晚期病人:
患者试图在较高的口 慢性疲劳导致 患者动用辅助呼吸肌和膈肌呼吸,
腔内气压下进行呼气, 活动耐量下降 从而使气道更开放
以改善气流
晚期病人:膈肌 “平坦” ,持续吸气进一步压 缩膈肌à 向内拉季肋部胸壁
胡佛征 (吸气时,胸廓下侧季肋部内收)
缩唇呼吸
肌肉无力 & 消瘦
端坐呼吸 (调动胸肌)
颈部肌肉收
缩(胸锁乳
突肌、斜角
肌)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Findings on Investigations
Chronic Obstructive Pulmonary Disease (COPD)
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
Airflow obstruction
Lung tissue damage
↓ ventilation of alveoli
Blood perfusing ill- ventilated alveoli does not receive normal amounts of oxygen
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction)
No elastic recoil to push air out of lungs
Loss of lung parenchyma and vasculature ↓ surface area for gas exchange
↓ diffusion capacity
(on spirometry)
Hypoxemia: PaO2 < 70mmHg (on ABGs)
Abbreviations:
• FEV1: Forced expiratory volume in 1 second
• FVC: Forced vital capacity
• TLC: Total lung capacity
• VC: Vital Capacity
Investigations for COPD :
• Spirometry (Pulmonary function test)
Total expiration time takes longer than normal
FEV1/FEV < 0.7
(on spirometry)
Lungs don’t fully empty
More air trapped within lungs (hyperinflation)
More CO2 remains and diffuses into the blood
Hypercapnia: PaCO2 > 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" />
45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" title="COPD: 临床表现
作者: Yan Yu 审稿人:Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人:Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
/012
(如a1-抗胰蛋白酶缺乏) 阻止肺组织损伤的能力↓
+,-.
(如长期吸烟、环境污染、感染)
肺内产生自由基
34*5
肺抗蛋白酶的失活
↑氧化应激,炎性细胞因子,蛋白酶功能
支气管的持续、反复损伤
炎性细胞浸润, 杯状细胞增殖, 气道上皮纤毛 尤其中性粒细 黏液产生↑ 细胞死亡
气道弹性↓ (弹性回缩
肺实质的蛋白水解破坏↑ 维持气道开放 肺泡永久性异常
的结构支持↓ 扩张
胞 力)
肺气体潴留 气道狭窄与 肺过度 肺大泡
气道黏液潴留,成为感染 狭窄 病灶
塌陷 充气
肺气肿
(容易肺泡 破裂)
气道纤维化和
%&'()*
慢性阻塞性肺疾病(COPD)
临床表现 并发症 (参阅相关幻灯片) (参阅相关幻灯片)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Clinical Findings Lung tissue
Chronic Obstructive Pulmonary Disease (COPD)
damage
↓ elastic recoil to push air out of lungs on expiration
Lungs don’t fully empty, air is trapped in alveoli (lung hyperinflation)
↑ lung volume means diaphragm is tonically contracted (flatter)
If occurring around airways
Airflow obstruction
↑ mucus production
↓ number of epithelial ciliated cells to clear away the mucus (the cells have been killed by airway inflammation)
Chronic cough with sputum
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
↓ perfusion of body tissues (i.e. brain, muscle)
Fatigue; ↓ exercise tolerance
Total expiration time takes longer than normal
Prolonged expiration
More effort needed to ventilate larger lungs
Respiratory muscles must work harder to breathe
Turbulent airflow in narrower airways is heard on auscultation
Expiratory Wheeze
Diaphragm can’t flatten much further to generate deep breaths
To breathe, chest wall must expand out more
Dyspnea
Shortness of breath, especially on exertion
Breathes are rapid & shallow
If end-stage:
Chronic fatigue causes deconditioning
Muscle weakness & wasting
Barrel chest
If end-stage: diaphragm will be “flat”. Continued
Patient tries to expire against higher mouth air pressure, forcing airways to open wider
Pursed-lip breathing
Patient breathes with accessory muscles as well as diaphragm to try to improve airflow
inspiratory effort further contracts diaphragmà pull the lower chest wall inwards
Hoover’s sign
(paradoxical shrinking of lower chest during inspiration)
Tripod sitting position (activates pectoral muscles)
Neck (SCM, scalene) muscles contracted
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$
慢性阻塞性肺疾病 (COPD) 如果出现在气道周围 气流阻塞
肺不能完全排空
气体,气体潴留
于肺泡(肺过度
充气)
总呼气时长大于 正常时长
呼气相延长
肺组织损伤
呼气时,将空气排出肺外 的弹性回缩力↓
肺不能完全排空气体,
气体潴留于肺泡内
(肺过度充气)
肺容积↑,膈肌紧张 性收缩(膈肌平坦)
呼气时,胸膜腔正压挤压气道 à 气道阻塞↑
肺泡通气↓ 血液氧合↓ (低
氧血症)
身体组织灌注 量↓ (比如脑、 肌肉)
疲劳; 运动耐量↓
黏液生成↑ 清除黏液的上皮纤
毛细胞数量↓ (受 气道炎症损伤)
慢性咳嗽伴咳 痰
作者: Yan Yu
审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳),
Zesheng Ye (叶泽生)
* 发表时担任临床医生
容积较大 的肺需要
更加努力 才能通气
呼吸肌必须
更用力才能 呼吸
听诊闻及狭窄气
道中的湍流气流
呼气喘鸣音
呼吸困难 气促,尤其是劳累
膈肌无法进一步收缩以
产生深呼吸
呼吸浅快
为了呼吸,
胸壁必须延
展得更大
桶状胸
晚期病人:
患者试图在较高的口 慢性疲劳导致 患者动用辅助呼吸肌和膈肌呼吸,
腔内气压下进行呼气, 活动耐量下降 从而使气道更开放
以改善气流
晚期病人:膈肌 “平坦” ,持续吸气进一步压 缩膈肌à 向内拉季肋部胸壁
胡佛征 (吸气时,胸廓下侧季肋部内收)
缩唇呼吸
肌肉无力 & 消瘦
端坐呼吸 (调动胸肌)
颈部肌肉收
缩(胸锁乳
突肌、斜角
肌)
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Findings on Investigations
Chronic Obstructive Pulmonary Disease (COPD)
Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Naushad Hirani* Juri Janovcik* * MD at time of publication
Airflow obstruction
Lung tissue damage
↓ ventilation of alveoli
Blood perfusing ill- ventilated alveoli does not receive normal amounts of oxygen
During expiration, positive pleural pressure squeezes on airwaysà↑ obstruction)
No elastic recoil to push air out of lungs
Loss of lung parenchyma and vasculature ↓ surface area for gas exchange
↓ diffusion capacity
(on spirometry)
Hypoxemia: PaO2 < 70mmHg (on ABGs)
Abbreviations:
• FEV1: Forced expiratory volume in 1 second
• FVC: Forced vital capacity
• TLC: Total lung capacity
• VC: Vital Capacity
Investigations for COPD :
• Spirometry (Pulmonary function test)
Total expiration time takes longer than normal
FEV1/FEV < 0.7
(on spirometry)
Lungs don’t fully empty
More air trapped within lungs (hyperinflation)
More CO2 remains and diffuses into the blood
Hypercapnia: PaCO2 > 45
(on ABGs)
Ventilation- perfusion mismatch
High A-a gradient
(calculated from ABGs)
Low, flat diaphragm, >10 posterior ribs
(on frontal CXR)
High TLC and VC
(on spirometry)
• •
PaO2: partial pressure of O2 in arterial blood PaCO2: partial pressure of CO2 in arterial blood
• In the setting of fever and productive cough, especially if lung field opacifications are seen on CXR: consider sputum gram stain and culture to rule out pneumonia.
Air does not block X-ray beams, will appear black on X-ray film
Chronic hypercapnia makes breathing centers less sensitive to the high PaCO2 stimulus for breathing, & more reliant on the low PaO2 stimulus
(“CO2 retention”)
Give O2 carefully to these patients (high PaO2 may suppress patients’ hypoxic respiratory drive, ↓ their breathing, & ↑↑↑ PaCO2)
↑ retrosternal air space
(on lateral CXR)
Hyper-lucent
(darker) lung fields, ↓ lung markings (on frontal CXR)
• Arterial Blood Gasses (ABGs)
• Chest X-Ray (CXR): frontal and
lateral
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"#$ 气流阻塞
肺泡通气↓ 呼气时,胸膜腔正压挤压气 道à 阻塞↑
作者: Yan Yu 审稿人: Jason Baserman, Jennifer Au, Naushad Hirani*, Juri Janovcik* 译者:Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
慢性阻塞性肺疾病 (COPD)
肺组织损伤
没有弹性回缩力将
气体排出肺
肺实质与血管分布减少导 致气体交换面积↓
弥散功能↓ (肺功能检查)
更多的CO2残留 并扩散到血液中
高碳酸血症: PaCO2 > 45
(动脉血气)
血流灌注通气不良的肺泡
时无法获得足够的氧气
总呼气时长较正常长
FEV1/FEV < 0.7
(肺功能检查)
肺无法完全排空
更多空气潴留在肺部
(肺过度充气)
低氧血症: PaO2 < 70mmHg
(动脉血气)
通气-灌注不匹配
肺泡-动脉氧分压差↑ (可通过动脉血气分析计算得出)
横膈低平, 下移至第10肋后端 及以下部位 (胸部正位片)
TLC与VC增大 (肺功能检查)
缩写: • • FEV1: 1秒用 •
VC:肺活量
PaO2: 动脉血 力呼气量 氧分压
空气不会阻挡X射线, 在X光片上呈现为黑色
慢性高碳酸血症使呼吸中枢对PaCO2 刺激呼吸的敏感性下降 & 更依赖于低PaO2的刺激 (“二氧化碳潴留”)
给患者吸氧时需注意(高PaO2
可能会抑制患者低氧时对呼吸的 刺激,使呼吸驱动↓ & PaCO2↑↑↑ )
• FVC: 用力肺 • 活量
• TLC:肺总量 慢阻肺相关检查 :
PaCO2: 动脉 血二氧化碳 分压
胸骨后间隙↑
(胸部侧位片) 肺纹理↓
• 肺功能检查
• 动脉血气分析(Arterial Blood Gasses, ABGs)
• 胸部正侧位片
• 当患者发热和湿咳,特别是胸片上见肺野不清晰时:
肺透亮度↑, (胸部正位片)
考虑进行痰革兰氏染色及痰培养以排除肺炎可能
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
COPD: Complications Lung inflammation
Chronic Obstructive Pulmonary Disease (COPD)
Airway obstruction ↓ inhaled air in alveoli and terminal bronchioles
Rupture of emphasematous bullae on surface of lung
Inhaled air leaks into pleural cavity and is trapped there
Pneumothorax
Feeling a loss of control over one’s life, and hopelessness for the future
Goblet cell proliferation, ↑ mucus production
Death of airway
epithelium ciliated cells
↓ oxygenation of the blood passing through the lungs
Chronic hypoxemia
Kidneys compensate by ↑ erythropoietin (EPO) production
↑ Hemoglobin and red blood cell synthesis
Polycythemia (secondary)
Hypoxic alveoli cause the pulmonary arterioles perfusing them to reflexively vasoconstrict
Since most alveoli in the lungs are hypoxic, hypoxic vasoconstriction occurs across entire lung
Vasoconstriction ↑ blood pressure within lung vasculature
Pulmonary hypertension
↑ workload of the right ventricle (to pump against higher pressures)
To compensate, the right ventricle progressively hypertrophies and dilates, but over time its output ↓
Cor pulmonale
(Right heart failure in isolation, not due to Left heart failure)
Mucus trapped in airways, serve as nidus for infection
Acute exacerbation of COPD (AECOPD)
Pneumonia
The chronic, systemic inflammation in COPD is a hyper-metabolic state that consumes calories
Macro-nutrient deficiency
Trouble with respiration lead to inactivity and deconditioning
Wasting, muscle atrophy
More inactivity and deconditioning perpetuates the cycle
Depression
Author: Yan Yu Reviewers: Jason Baserman Naushad Hirani* Juri Janovcik* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 7, 2013 on www.thecalgaryguide.com
COPD: !"# 肺部炎症
杯状细胞增殖, 气道上皮纤毛 粘液产生↑ 细胞死亡
黏液潴留呼吸道,成为感
染的病灶
慢性阻塞性肺疾病 (COPD) 气道阻塞à 吸入肺泡和终末细
肺大疱破裂
吸入的空气渗入
并潴留于胸腔
气胸
感觉生活失控,对未
来感到绝望
抑郁
作者: Yan Yu 审稿人: Jason Baserman, Naushad Hirani*, Juri Janovcik* 译者: Zihong Xie (谢梓泓) 翻译审稿人: Yonglin Mai (麦泳琳), Zesheng Ye (叶泽生) * 发表时担任临床医生
支气管的空气 ↓
流经肺的血液进行气 缺氧的肺泡à灌注肺泡的肺小动
慢性阻塞性肺疾 病急性加重期 (AECOPD)
肺炎
体交换↓ 慢性低氧血症
肾脏合成促红细胞 生成素进行代偿↑
血红蛋白与红 细胞合成↑
红细胞增多症 (继发性)
脉发生反射性血管收缩
肺大部分肺泡缺氧à整个肺 都出现缺氧性血管收缩
肺血管收缩 à 肺血管压力↑ 肺动脉高压
↑ 右心室负荷(泵血时对抗高压) 为了代偿,右心室逐渐肥大和扩张,
但随着病程进展,右心室输出量 ↓
肺心病 (单独出现右心衰竭,非左心衰)
COPD所致的慢性全身 呼吸困难导致活 性炎症会使机体处于高 动量减少和活动
代谢状态,消耗能量 耐量降低
宏量营养 素缺乏症
消瘦,肌肉萎缩
运动量下降和活动耐量
的降低造成恶性循环
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年1月7日发布于 www.thecalgaryguide.com
" />
哮喘急性发作-发病机制和治疗
 Kang,Usama Malik,Lian Szabo*
译者:Yonglin Mai (麦泳琳) 翻译审核人:Zesheng Ye (叶泽生) * 发表时担任临床医生
下呼吸道炎症
免疫系统激活:气道上皮趋化因子、淋巴细胞和巨噬细胞激活, 白三烯产生↑ 炎症介质释放
哮喘轻中度急性发作: PEF ≥ 预计值50%
疗效良好: 症状缓 解, PEF ≥ 80%
患者日常在家 服用糖皮质激 素及必要时使 用SABA
支气管狭窄
残气量↑ 及PaCO2↑
气体潴留↑,肺 泡内压力 ↑
奇脉
气体通过 发炎的呼 吸道产生 的刺激↑
咳嗽和喘息
Notes
呼吸 困难
黏膜水肿会导 致气流湍急
喘息
吸O2使SpO2 ≥ 92%, 给予SABA & 糖皮质激素 治疗
重度急性发作: PEF ≤预计值 50%
呼吸困难
呼吸急促 呼吸衰竭
意识丧失
↓ 向肺泡传送 空气氧含量
血氧饱和度↓
•
•
Asthma哮喘: Airway hyper- responsiveness causing airflow obstructions气道高反应性引起气流受 限
Acute Exacerbation (Asthma)哮喘急性 发作: An episode of increased symptoms due to decreases in airflow气流减少而 引起一系列症状加重
Abbreviations
• PaCO2动脉二氧化碳分压:Partial
pressure of CO2 in arterial blood
• PEF最大呼气流量/呼气流量峰值: Peak
expiratory flow
• SABA短效beta-2受体激动剂: Short-
acting beta-2 agonists
• SpO2血氧饱和度: Blood oxygen
saturation level
昏睡
气胸
中枢性紫绀 心动过速
患者宣教: 正确服用药物,使用 药物吸入装置 &全科医生密切医学随 访
吸 O 使 SpO ≥ 2 2
症状恶化和/或呼吸衰竭 :及时气 管插管, 送往ICU, 给予SABA, 糖皮 质激素 & 硫酸镁
取决于气胸严 重程度: 密切观 察或者置入胸 腔引流管
93%, 给予 SABA, 糖皮质激素 & 硫 酸镁
图注:
病理生理
机制
体征/症状/实验室检查
并发症
2018年 2月6日发布于 www.thecalgaryguide.com")
Asthma clinical findings

Author: Yan Yu Reviewers: Jason Baserman Jennifer Au Yonoglin Mai (麦泳琳) Naushad Hirani* * MD at time of publication
Variable, sporadic airway obstruction in response to triggers
Associated allergic eosinophil response
Eosinophils infiltrate: Skin
If severe:
↓ ventilation of alveoli
↓ oxygenation of blood (hypoxemia)
During expiration, positive pleural pressure squeezes on airwaysà↑↑ airway obstruction
Heart rate to improve
perfusion of tissue
Tachycardia
Respiratory centers rate of breathing to
compensate
Tachypnea
Gas is trapped within alveolià hyperinflates lungs
Ventilating larger lungs needs more effort
Patients need to voluntarily contract
their expiratory muscles faster and more forcefully to effectively expire
Narrower airways àturbulent
airflow, heard on auscultation
Expiratory Wheeze (high-pitched expiratory sound)
Nose
Rhinitis/ sinusitis
Runny nose, sneezing, etc
Atopic dermatitis
Skin rash, hives
Eyes
Conjunctivitis
Red itchy eyes, visual blurring
Episodic
dyspnea
(shortness of breath)
Chest tightness
During severe attacks:
Note: Asthma attacks often have two phases:
• An immediate attack (within 0-2 hours of the trigger, due to acute release of histamine from mast cells)
• A delayed attack (due to eosinophil infiltration of airways, presents within 3-4 hours after exposure to the trigger, peaks within 6-8 hours, and resolves within 24 hours).
Keep the possibility of a delayed attack in mind when treating patients in Emergency!
Note: Symptoms often worse at night or early in the morning.
Note: Asthma should be suspected in children experiencing dyspnea with multiple episodes of Upper Respiratory Tract Infections or Croup.
Patient compensates by activating accessory respiratory muscles to ↑ thoracic volume
Visible contraction of
neck muscles (Scalene, sternocleidomastoids)
↑↑↑ airway obstruction on
expiration, lungs take more time to empty
Prolonged expiratory phase of breathing
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 17, 2012 and updated Dec 4, 2021 on www.thecalgaryguide.com")
Chronic Cough Pathogenesis_2021

Infection
IP; likely chronic ↑ cough receptors commonly pertussis- related or post-viral
Asthma
↑ EDN
↑ MBP levels in RT
Neoplasm
Bronchiectasis
COPD
GERD
Allergic Rhinitis
↑ sputum production
and accumulation
Damage from chronic inflammation causes poor mucus clearance
Inhalants trigger ↑ cytokines ↑ mucus
Aspiration of refluxed microdroplets
Irritation by post- nasal drip
↑ inflammatory mediators in RT
Mechanical obstructions (i.e. mediastinal masses, neoplasms)
Foreign body Presence irritation of irritants
Stimulation of sensory nerve receptors expressed on nerve endings penetrating the epithelia of the upper RT
Abbreviations:
• RT: respiratory tract
• IP: indefinite
pathophysiology
• GERD: Gastro-esophageal
reflux disease
• EDN: Eosinophil-derived
neurotoxin
• MBP: Major basic protein
• COPD: Chronic
Obstructive Pulmonary Disease
Complications: Syncope, insomnia, hemoptysis, rib fractures
Slowly adapting receptors
Respond to mechanical forces during breathing
Stimulation of the vagus nerve
Activation of nucleus tractus solitarius in central respiratory generator (brainstem)
Generation of efferent cough signal
Chronic cough: Cough of over 8 weeks duration with no dyspnea or fever
C-fibre receptors
Respond to chemical stimuli (bradykinin, capsaicin, acid/alkaline solutions, mannitol, hypertonic saline, and other inhaled irritants)
Authors: Arsalan Ahmad Lance Bartel Reviewers: Midas (Kening) Kang Usama Malik Ciara Hanly Yonglin Mai (麦泳琳) Yan Yu*, Eric Leung* * MD at time of publication
Rapidly adapting receptors
Responds to mechanical stimuli, such as physical obstruction of the airways
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 06, 2018, updated Dec 4, 2021 on www.thecalgaryguide.com")
mechanical-bowel-obstruction-and-ileus-pathogenesis-and-clinical-findings

Post-abdominal surgery
Authors: Yan Yu, Wayne Rosen* Reviewers: Nicole Burma, Jason Baserman, Jennifer Au, Maitreyi Raman* * MD at time of publication
Adhesions Note:
• Complete obstruction typically
presents with acute abdominal
pain and related symptoms • Incomplete obstructions can present with either acute or
Congenital abnormality GI neoplasms
If partial obstruction: ↓ frequency of bowel movements
Since gas/air sounds hollow to percussion Abdomen tympanic to percussion
Mechanical obstruction: physical blockage of bowel lumen
Inflammatory bowel disease (IBD)
Gas (from swallowed air, bacterial fermentation, & CO2 made via HCO3- neutralization) & ingested gastro- intestinal (GI) contents accumulate before obstruction
Accumulated GI contents contain salts and other osmotically active solutes that osmotically draw water into the GI tract
Continued ↑ bowel distention & ↑ luminal pressure over time
↑ pressure squeezes shut intestinal blood vesselsà↓ bowel perfusion
chronic abdominal pain
If complete obstruction: Obstipation (no flatus) & absent bowel movements
Irritation of autonomic nerves in visceral peritoneum
Lower effective arterial blood volumeàdehydration
Continued peristalsis proximal to obstruction continues to push GI contents against the obstruction
If obstruction is proximal (closer to mouth), higher luminal pressure may force regurgitation of GI contents
Bloating, cramping, anorexia Diffuse visceral abdominal pain
Flat/low jugular venous pressure (JVP), resting tachycardia, orthostatic hypotension
Severe abdominal pain (may come in waves), peritonitis, guarding, rigidity
Hyperactive bowel sounds (proximal to obstruction) or absent bowel sounds (ileus)
Nausea/vomiting
Bowel ischemia and infarction, tissue necrosis, possible perforation +/- bacterial invasion (see relevant slides)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published December 15, 2021 on thecalgaryguide.com")
obstruccion-del-intestino-delgado-hallazgos-en-los-rayos-x

obstruccion-intestinal-mecanica-e-ileo-patogenesis-y-hallazgos-clinicos

Langerhans Cell Histiocytosis
 CD1a+/CD207+ (Langerhans cell phenotype surface receptors) dendritic cells in tissue(s)
Somatic BRAFV600E mutation: BRAF is a kinase in the MAPK pathway
Other somatic (non- reproductive cell) mutations
Idiopathic (unknown cause)
Mutation(s) can occur in one of these precursor cell types*
Hematopoietic stem cell (earliest cell of blood cell differentiation) in bone marrow
Committed dendritic cell (type of myeloid antigen-presenting cell) precursor in bone marrow or blood
Committed dendritic cell precursor in tissue
Constitutive activation of the MAPK pathway (signalling pathway that regulates variety of cellular processes) in one of these precursor cell types
*Note: Based on the “misguided myeloid differentiation” modelàthe earlier the mutation(s) occur in the myeloid cell differentiation pathway, the more severe the disease.
Langerhans Cell Histiocytosis
Accumulation of abnormal CD1a+/CD207+ dendritic cells (Langerhans Cell Histiocytosis cells or LCH cells) with an inflammatory background in one or more organs
Authors:
Ran (Marissa) Zhang Reviewers:
Mehul Gupta
Kiera Pajunen
Yan Yu*
Lynn Savoie*
* MD at time of publication
↑ recruitment & activation of T cells, macrophages, eosinophils in tissue(s) around the body
↓ CCR7 & CXCR4 (chemokine receptors) expression on LCH cellsàinhibits migration of LCH cells to lymph nodes
↑ BCLXL (an apoptosis regulator protein) expression on LCH cellsà inhibits apoptosis of LCH cells
Immune cell infiltration & ↑ pro-inflammatory chemokine/cytokine release à dysregulated local & systemic inflammation
Accumulation of LCH cells in tissue(s) around the body
Inflammatory lesion (an area of abnormal tissue) formation in one or more organs:
In pituitary stalk
Mass effectà
obstruction of antidiuretic hormone (complex mechanisms)
In liver
Invasion & accumulation of cells foreign to liverà expands liver
Chronic local inflammation
Scarring of bile ducts
↓ bilirubin clearance from liveràbuildup into serum
↑ serum bilirubin
Jaundice
In cortical bone Cytokine production
à↑ osteoclast
(cells that break down bone) activity
↑ rate of bone loss
Osteolytic bone lesions
In bone marrow
Unclear mechanism but likely due to macrophage activation
↑ phagocytosis (ingestion & destruction) of blood cells
In spleen
Invasion & accumulation of cells foreign to spleen
Forms aggregates that expand the red pulp (functions as the blood filter in spleen)
Splenomegaly
In skin
Unclear mechanisms
Variable presentations: most commonly pinpoint erythematous (red) papules or erythematous plaques with crusting & scaling
Hepatomegaly • BRAF- B-Raf proto-oncogene, serine/threonine kinase
• CCR7- C-C motif chemokine receptor type 7
• CD1a- Cluster of differentiation 1A
• CD207- C-type lectin domain family 4 member k • CXCR4- C-X-C chemokine receptor type 4
• LCH- Langerhans Cell Histiocytosis
• MAPK- Mitogen-activated protein kinase
Diabetes Insipidus
Abbreviations:
• BCLXL- B-cell lymphoma-extra large
Anemia, thrombocytopenia &/or neutropenia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 13, 2022 on www.thecalgaryguide.com")
NSAIDs and the Kidney mechanism of action and side effects
 or angiotensin II receptor blockers (ARB)
AECi and ARBs act to ↓ renin- angiotensin-aldosterone system (RAAS) activation
Reduced angiotensin (AT) 2 activity at its receptors on efferent arteriole of the nephron
Net vasodilation of efferent arterioles ↓ in glomerular pressure
↓ blood perfusing kidney tissueà↑ hypoxemia & renal ischemia
Pre-existing ↓effective arterial blood volume (EABV) from
dehydration, GI loss, diuretics, CKD, CHF, cirrhosis, etc.
Decreased EABV triggers endogenous renal autoregulation, resulting in norepinephrine (NE) mediated vasoconstriction of afferent arteriole of the nephron
Net ↓ in renal blood flow and ↓ in glomerular pressure
↓ volume of blood filtered by the glomeruli per unit time
Non-steroidal anti-inflammatory drugs (NSAIDs)
Inhibition of Cyclooxygenase COX-1 (expressed in kidney) and COX-2 (expressed in kidney and sites of inflammation)
↓ Renal prostaglandin (PG) synthesis: local hormones involved in renal homeostasis
NSAID induced nephrotoxicity:
associated with chronic usage independent of dosage
(see Calgary Guide slide on NSAIDs and the Kidney: NSAID induced nephrotoxicity)
↓ intrarenal PG reduces inhibitory effects of PG over ADH in cortical colleting duct (CCD) of the kidneyà↓ antagonism on ADH activity
↑ ADH activity causes insertion of more
aquaporins (water channels) in the collecting duct of renal tubules
Net ↑ in volume of water reabsorbed into the blood
↓ vasodilatory effect of PG at the afferent arteriole of the nephron
↓ Glomerular filtration rate (GFR)
↓ PG signalling results in ↓ renin secretion at juxtaglomerular apparatus
Low renin levelsà↓ conversion of angiotensinogen into its AT1 form and, by extension, ACE mediated conversion of AT1 to AT2
↓ ACE 2 signalling leads to ↓ levels of aldosterone in the serum
↓ Na+ and K+ channel insertion on apical surface and ↓ Na/K ATPase activity on basolateral surface of principal cells
↓ K+ excretion into urine, and ↓ Na+ reabsorption
back into the blood, at the late DCT and collecting duct of the kidney
Pre-renal Acute Kidney Injury (AKI): kidney injury due to renal hypoperfusion
Prolonged and/or severe ischemia causes cell death and aggregation of tubular epithelial cells of the kidney with subsequent inability to reabsorb luminal Na+
Renal dehydration predisposes
precipitation of uromodulin protein
Renal tubules mold uromodulin into cylindrical structures known as “casts”. Casts that contain only uromodulin protein are known as “hyaline casts”
Hyaline cast seen on urinalysis
Hypoperfusion of the kidney activates the renin- angiotensin- aldosterone system (RAAS)
↑ amount of sodium (Na) reabsorbed from the filtrate (less Na excreted)
Fractional excretion of Na <1%
Papillary necrosis: ureteral passage of sloughed ischemic tissue causing ureteral obstruction
Acute tubular necrosis: a type of kidney injury causing damage to the tubules
Hypertension
Post-renal AKI: a type of kidney injury due to
obstruction of the urinary tract
Distal distal obstruction of the urinary tract causes fluid to accumulate within the kidneysàenlarging the kidneys
Renal Ultrasound shows hydronephrosis (enlarged kidneys)
Damaged tubule epithelial cells slough into the tubular lumen
Epithelial cell breakdown in the tubular lumen
releases uromodulin & other proteins, which aggregate into “casts” (cylindrical imprints of the renal tubule). The varied protein content of these casts result in them having a coarse, granular appearance
Damaged tubular epithelial cells are unable to properly reabsorb sodium
↓ amount of sodium (Na) reabsorbed from filtrate into the blood (more Na excreted)
Fractional excretion of Na >2%
True excess of free water relative to Na+ in the blood
Excess free water ↑ venous hydrostatic pressure (see Calgary Guide slide on edema for full mechanisms)
Pitting Edema
Hyperkalemia
Hyponatremia
Coarse granular casts seen on urinalysis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 29, 2022 on www.thecalgaryguide.com")
obstructive-sleep-apnea-pathogenesis-and-clinical-findings
![Obstructive Sleep Apnea: Pathogenesis and clinical findings
Vascular Factors: During recumbent sleep, more bodily fluids enter the head and neck area (compared to when the patient is standing/sitting)
↑ volume of head/neck tissue surrounding the upper airwayà possible airway obstruction
Authors: Ciara Hanly Austin Laing Alexander Arnold Reviewers: Steven Liu Amogh Agrawal Yonglin Mai (麦泳琳) Naushad Hirani* Yan Yu* *MD at time of publication
Neuromuscular Factors: Sleep onset and/or the sleeping state reduces the drive of respiratory muscles to breathe
↓ Upper airway neuromuscular activityà↓ upper airway caliber, ↑ upper airway resistance, ↑ upper airway collapsibility during sleep
Structural Factors: Obesity, tonsillar or adenoid hypertrophy, macroglossia, ↑ neck circumference, craniofacial abnormalities
Excess pressure on upper airway, or deformity to that area, ↑ risk of upper airway collapse
Polysomnography
Absence of airflow but persistent ventilatory effort
Hypopnea or Apnea
Paradoxical breathing Chest wall draws in and abdomen expands during inspiration
Ventilatory effort persists against closed airway
No air entry due to collapsed upper airway
↑ Negative intrathoracic pressure
↑ Venous return to right atrium
Stretching of right atrial myocardium à secretion of atrial natriuretic peptide (ANP)
ANP inhibits epithelial Na+ channels (ENaC) in the collecting ducts of the kidney from reabsorbing Na+ à Na+ excretion
↑ Na+ excretionà↑ water excretion
Nocturia
Complete or partial upper airway obstruction during sleep
↑ PCO2 & ̄ PO2
in the lungsà ̄ diffusion gradient of CO2 & O2 between lungs & arteries
↑ PaCO2,, ̄ PaO2
Respiratory acidosis (↑ [H+] in blood)àactivation of vascular endothelial voltage gated K+ channels
Cerebral blood vessel dilation to provide adequate O2 to brain
Morning Headaches
Activation of central (medulla oblongata) & peripheral (carotid body) chemoreceptors
↑ Respiratory drive à ↑ activation of respiratory muscles (ventilatory effort )
Transient arousal from sleep
↑ sympathetic nervous system activityà arterial vasoconstriction
↑ systemic vascular resistance
Systemic Hypertension
↑ intraluminal pressure within blood vesselsàadaptive vascular endothelial and smooth muscle changes
Artery walls thicken, harden and lose elasticityà ̄ perfusion to end organs (such as the brain)
Ischemic stroke
Hypoxia during the day and night
↑ pulmonary vascular resistance
Pulmonary Hypertension
Right heart pumps against higher pulmonary pressure àcardiomyocytes undergo concentric hypertrophy over time
Cor Pulmonale
(Right heart failure due to pulmonary hypertension, separate from left heart failure)
Respiratory muscles overcome upper airway obstructionà airway patency restored
Sleep fragmentation
̄ Daytime cognitive performance and attentiveness
↑ Risk of motor vehicle accidents
Daytime Sleepiness
Eg. Epworth Sleepiness Scale >10
Abbreviations:
PCO2: partial pressure of carbon dioxide PO2: partial pressure of oxygen PaCO2: partial pressure of carbon dioxide in arteries PaO2: partial pressure of oxygen in arteries
Ventilatory response overcompensatesà breathe out more CO2 than is required for homeostasisà ̄ PaCO2
̄ respiratory driveà ̄ ventilatory effort
Resuscitative Gasping
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 19, 2013, updated May 31, 2022 on www.thecalgaryguide.com
阻塞性睡眠呼吸暂停:发病机制及临床表现
作者:Ciara Hanly, Austin Laing, Alexander Arnold 审稿人: Steven Liu, Amogh Agrawal, Naushad Hirani*,Yan Yu* 译者: Zesheng Ye(叶泽生) 翻译审稿人: Yonglin Mai(麦泳琳) *发表时担任临床医生
神经肌肉因素: 睡眠状态下, 患者无法通过 适当增加上气道肌张力来维持气道通畅
上气道神经肌肉活动 ̄à上气道直径 ̄, 上气道 阻力↑, 睡眠时上气道塌陷
结构(解剖)因素: 肥胖、扁桃体或腺样体 肥大, 舌体肥大, 颈围增大, 颅面部畸形
上气道压力过大或上气道畸形, 上气道塌陷 的风险 ↑
血管因素: 仰卧位睡觉引起 夜间嘴侧液体移位
周围组织与压力 ↑à上气道阻塞
多导睡眠描记术
没有气流,但持
续通气
呼吸浅慢或 呼吸暂停
反常呼吸 吸气时胸壁凹陷, 腹部膨隆
持续通气以抵抗气道 闭合
上气道塌陷导致空气进
入气道受阻
腹膜腔负压↑ 静脉血回流右心室阻力↑
右心房心肌细胞拉伸 à心房利钠肽分泌 (ANP)
ANP抑制肾集合管的上 皮Na+通道(ENaC)对 Na+重吸收à Na+排出
Na+排出量↑ à 水排出量 ↑
睡眠时全部
或部分上呼
吸道阻塞
肺内PO2 ̄ 且 PCO2↑ à CO2 及 O2在肺和动脉 间的扩散梯度 ̄
↑ PaCO2, ̄ PaO2
呼吸性酸中毒 (血液中 [H+] ↑) à激活血管内皮电压
门控 K+
脑血管扩张为大 晨间头痛 脑提供足够的 O2
激活中央(延髓)和外周(颈动脉体)的化学感受器 呼吸驱动↑à呼吸肌活动 (呼吸做功 )↑
短暂的睡眠唤醒
通道 交感神经系统活动↑
全天缺氧 肺血管阻力↑
肺动脉高压
右心泵血以抵抗肺 动脉高压à 随着时 间推移,心肌向心 性肥大
肺心病(区别于左
心衰,右心衰是肺
动脉高压所致)
呼吸肌克服上气道阻力à 气道 明显恢复
睡眠过程不连续
白天的认知功能
及注意力 ̄
机动车辆事故风险↑
白天嗜睡
à 动脉收缩 全身血管阻力↑
高血压
血管内压力↑ à 血 管内皮和平滑肌发生 适应性改变
动脉壁增厚、硬化、失 去弹性à器官血液灌 注量 ̄ (如脑部)
缩写: PCO2:二氧化碳分压 PO2:氧分压 PaCO2:动脉二氧化 碳分压 PaO2:动脉血氧分压
通气过度 à呼出CO2 ↑ à PaCO2 ̄
呼吸驱动 ̄à 呼吸做功 ̄
复苏性鼾音
夜尿症
如:伊普沃斯嗜睡评分
>10
缺血性卒中
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年8月19日发表 www.thecalgaryguide.com, 2022年5月31日更新](https://calgaryguide.ucalgary.ca/wp-content/uploads/2014/09/OSA-2021-1.jpg "Obstructive Sleep Apnea: Pathogenesis and clinical findings
Vascular Factors: During recumbent sleep, more bodily fluids enter the head and neck area (compared to when the patient is standing/sitting)
↑ volume of head/neck tissue surrounding the upper airwayà possible airway obstruction
Authors: Ciara Hanly Austin Laing Alexander Arnold Reviewers: Steven Liu Amogh Agrawal Yonglin Mai (麦泳琳) Naushad Hirani* Yan Yu* *MD at time of publication
Neuromuscular Factors: Sleep onset and/or the sleeping state reduces the drive of respiratory muscles to breathe
↓ Upper airway neuromuscular activityà↓ upper airway caliber, ↑ upper airway resistance, ↑ upper airway collapsibility during sleep
Structural Factors: Obesity, tonsillar or adenoid hypertrophy, macroglossia, ↑ neck circumference, craniofacial abnormalities
Excess pressure on upper airway, or deformity to that area, ↑ risk of upper airway collapse
Polysomnography
Absence of airflow but persistent ventilatory effort
Hypopnea or Apnea
Paradoxical breathing Chest wall draws in and abdomen expands during inspiration
Ventilatory effort persists against closed airway
No air entry due to collapsed upper airway
↑ Negative intrathoracic pressure
↑ Venous return to right atrium
Stretching of right atrial myocardium à secretion of atrial natriuretic peptide (ANP)
ANP inhibits epithelial Na+ channels (ENaC) in the collecting ducts of the kidney from reabsorbing Na+ à Na+ excretion
↑ Na+ excretionà↑ water excretion
Nocturia
Complete or partial upper airway obstruction during sleep
↑ PCO2 & ̄ PO2
in the lungsà ̄ diffusion gradient of CO2 & O2 between lungs & arteries
↑ PaCO2,, ̄ PaO2
Respiratory acidosis (↑ [H+] in blood)àactivation of vascular endothelial voltage gated K+ channels
Cerebral blood vessel dilation to provide adequate O2 to brain
Morning Headaches
Activation of central (medulla oblongata) & peripheral (carotid body) chemoreceptors
↑ Respiratory drive à ↑ activation of respiratory muscles (ventilatory effort )
Transient arousal from sleep
↑ sympathetic nervous system activityà arterial vasoconstriction
↑ systemic vascular resistance
Systemic Hypertension
↑ intraluminal pressure within blood vesselsàadaptive vascular endothelial and smooth muscle changes
Artery walls thicken, harden and lose elasticityà ̄ perfusion to end organs (such as the brain)
Ischemic stroke
Hypoxia during the day and night
↑ pulmonary vascular resistance
Pulmonary Hypertension
Right heart pumps against higher pulmonary pressure àcardiomyocytes undergo concentric hypertrophy over time
Cor Pulmonale
(Right heart failure due to pulmonary hypertension, separate from left heart failure)
Respiratory muscles overcome upper airway obstructionà airway patency restored
Sleep fragmentation
̄ Daytime cognitive performance and attentiveness
↑ Risk of motor vehicle accidents
Daytime Sleepiness
Eg. Epworth Sleepiness Scale >10
Abbreviations:
PCO2: partial pressure of carbon dioxide PO2: partial pressure of oxygen PaCO2: partial pressure of carbon dioxide in arteries PaO2: partial pressure of oxygen in arteries
Ventilatory response overcompensatesà breathe out more CO2 than is required for homeostasisà ̄ PaCO2
̄ respiratory driveà ̄ ventilatory effort
Resuscitative Gasping
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 19, 2013, updated May 31, 2022 on www.thecalgaryguide.com
阻塞性睡眠呼吸暂停:发病机制及临床表现
作者:Ciara Hanly, Austin Laing, Alexander Arnold 审稿人: Steven Liu, Amogh Agrawal, Naushad Hirani*,Yan Yu* 译者: Zesheng Ye(叶泽生) 翻译审稿人: Yonglin Mai(麦泳琳) *发表时担任临床医生
神经肌肉因素: 睡眠状态下, 患者无法通过 适当增加上气道肌张力来维持气道通畅
上气道神经肌肉活动 ̄à上气道直径 ̄, 上气道 阻力↑, 睡眠时上气道塌陷
结构(解剖)因素: 肥胖、扁桃体或腺样体 肥大, 舌体肥大, 颈围增大, 颅面部畸形
上气道压力过大或上气道畸形, 上气道塌陷 的风险 ↑
血管因素: 仰卧位睡觉引起 夜间嘴侧液体移位
周围组织与压力 ↑à上气道阻塞
多导睡眠描记术
没有气流,但持
续通气
呼吸浅慢或 呼吸暂停
反常呼吸 吸气时胸壁凹陷, 腹部膨隆
持续通气以抵抗气道 闭合
上气道塌陷导致空气进
入气道受阻
腹膜腔负压↑ 静脉血回流右心室阻力↑
右心房心肌细胞拉伸 à心房利钠肽分泌 (ANP)
ANP抑制肾集合管的上 皮Na+通道(ENaC)对 Na+重吸收à Na+排出
Na+排出量↑ à 水排出量 ↑
睡眠时全部
或部分上呼
吸道阻塞
肺内PO2 ̄ 且 PCO2↑ à CO2 及 O2在肺和动脉 间的扩散梯度 ̄
↑ PaCO2, ̄ PaO2
呼吸性酸中毒 (血液中 [H+] ↑) à激活血管内皮电压
门控 K+
脑血管扩张为大 晨间头痛 脑提供足够的 O2
激活中央(延髓)和外周(颈动脉体)的化学感受器 呼吸驱动↑à呼吸肌活动 (呼吸做功 )↑
短暂的睡眠唤醒
通道 交感神经系统活动↑
全天缺氧 肺血管阻力↑
肺动脉高压
右心泵血以抵抗肺 动脉高压à 随着时 间推移,心肌向心 性肥大
肺心病(区别于左
心衰,右心衰是肺
动脉高压所致)
呼吸肌克服上气道阻力à 气道 明显恢复
睡眠过程不连续
白天的认知功能
及注意力 ̄
机动车辆事故风险↑
白天嗜睡
à 动脉收缩 全身血管阻力↑
高血压
血管内压力↑ à 血 管内皮和平滑肌发生 适应性改变
动脉壁增厚、硬化、失 去弹性à器官血液灌 注量 ̄ (如脑部)
缩写: PCO2:二氧化碳分压 PO2:氧分压 PaCO2:动脉二氧化 碳分压 PaO2:动脉血氧分压
通气过度 à呼出CO2 ↑ à PaCO2 ̄
呼吸驱动 ̄à 呼吸做功 ̄
复苏性鼾音
夜尿症
如:伊普沃斯嗜睡评分
>10
缺血性卒中
图注:
病理生理
机制
体征/临床表现/实验室检查
并发症
2013年8月19日发表 www.thecalgaryguide.com, 2022年5月31日更新")
ascending-cholangitis-pathogenesis-clinical-findings

Bacteria ascends into biliary tract from duodenum via Sphincter of Oddi
Gallstone in the common bile duct
Stricture of biliary/hepatic ducts
Biliary / pancreatic duct malignancy
Biliary obstruction (partial bile duct obstruction)
↓ Excretion of bilirubin into
bileà ↑ bilirubin in blood
↑ Serum bilirubin
Deposition of bilirubin in the skin and mucous membranes
Jaundice*†
Parasites in bile duct
(E.g. Clonorchis)
Complication of endoscopic retrograde cholangiopancreatography (ERCP)
Bile accumulates in biliary tract
Bile duct dilation on ultrasound
Sludge (bile precipitants) impact bile ducts worsening obstruction
Obstruction & detergents in bile inflame ductal mucosa. Inflammation then spreads to adjacent structures
Stimulates phrenic (C3-C5) and foregut autonomic nerves (T5-T8)
Dull right upper quadrant pain*† radiating to back and right shoulder
↑ Intra-biliary pressure
Impaired forward flowà
↑ backflow of bile
Impaired bile secretion damages ductal epithelium of the biliary tract
Damaged ductal epithelium leaks ALP and GGT (enzymes) into blood
↑ Serum ALP and GGT
↑ Permeability of bile ductules
Reduced flushing of bile out to duodenum
Inflammatory response triggered
Fever*† ↑ WBCs
Tachycardia Hypotension† Confusion† Oliguria
Bacterial translocation from biliary tract into blood
Bacteremia
Massive systemic inflammatory response
Septic Shock
(see Distributive Shock slide)
* Charcot’s triad ~20% of cases | † Reynolds’ pentad ~7% of cases
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published November 18, 2015; Updated August 31, 2022 on www.thecalgaryguide.com")
chronic-pancreatitis-complications
 from acinar cells in exocrine pancreas
(early in disease course)
Proteins precipitate and form aggregates within pancreatic ducts
Accumulation of protein aggregates and localized fibrosis block pancreatic ducts
Rupture of acinar cells near blocked ducts → release of intracellular enzymes and fluid
Accumulation of enzyme- rich fluid within pancreas
Intra-pancreatic pseudocysts (differ from pseudocysts in acute pancreatitis, which are primarily extra-pancreatic)
Chronic Pancreatitis
Recurrent episodes of acute pancreatitis leading to irreversible fibroinflammatory pancreatic damage
Inflammatory cytokines are
continuously released from damaged pancreas over years
Cytokines damage endothelium of intra- and peri-pancreatic blood vessels (including splenic vein, which runs posteriorly behind pancreas and allows for its venous drainage)
Thin and weakened
vessel walls balloon outwards from pressure of blood flow
Pseudoaneurysms
Venous stasis (low blood flow) → ↑ concentration of clotting factors
Obstruction of peripancreatic ducts
Author: Ashar Memon Reviewers: Yan Yu*, Kiana Hampton, Sylvain Coderre* * MD at time of publication
Exocrine insufficiency
(↓ secretion of digestive enzymes, e.g., Lipase, into gastro-intestinal tract)
↓ digestion of foods and absorption of nutrients (including fats)
↓ absorption of fat-soluble vitamin D
Metabolic bone disease
(a group of disorders of decreased bone mineralization)
Blood vessels dilate and swell from increased blood flow
Gastric varices
Cytokines perpetually activate pancreatic stellate cells (stellate cells produce proteins that remodel extra- cellular matrix)
Pancreatic stellate cells increase amounts of collagen and other extra- cellular matrix molecules in pancreas → Fibrosis
Pancreatic proteolytic enzymes (e.g., trypsin) in fluid-filled pseudocysts digest walls of adjacent blood vessels
Fibrotic tissue and pseudocysts compress peripancreatic structures (including splenic vein)
Cytokines stimulate apoptosis of hormone- producing pancreatic Islet cells
(e.g., beta cells)
Endocrine insufficiency
(↓ production and secretion of pancreatic hormones)
Damaged endothelial cells of splenic vein trigger coagulation cascade
(See Calgary Guide slide on Coagulation Cascade)
Splenic vein thrombosis
↑ resistance to blood flow through splenic vein
Cytokines
stimulate apoptosis of acinar cells in exocrine pancreas
Malnutrition
↓ secretion of insulin
↓ cellular uptake and metabolism of glucose → hyperglycemia
Diabetes mellitus
Collateral blood vessels develop around stomach so blood can circumvent splenic vein and relieve splenic vein hypertension
Duodenal obstruction Biliary obstruction
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 18, 2022 on www.thecalgaryguide.com")
Granulomatosis with Polyangiitis Pathogenesis

Environmental exposures
Silica dust, cigarette smoke, infections (Staphylococcus aureus)
Genetic factors
Alpha-1 antitrypsin deficiency, proteinase 3 gene mutation
↑ Production of cytokines and antineutrophil cytoplasmic antibodies (ANCAs) (mechanism unknown) Cytokines bind to endothelial cells (that line blood vessels) and neutrophils, priming them
Proteinase 3 (PR3), an enzyme that degrades extracellular matrix proteins, migrates from neutrophil granules to neutrophil cell surface
Circulating ANCAs bind to PR3 on neutrophils
PR3 stimulates maturation of dendritic cells in lungs
Dendritic cells present antigen (PR3) to naïve CD4+ T cells in peripheral lymph nodes
T cells differentiate into type 1 and type 17 helper T cells (Th1 and Th17 cells)
Th1 and Th17 cells secrete cytokines (interferon γ (INF-γ) and tumor necrosis factor α (TNF-α)) in lungs
Secreted cytokines trigger macrophage maturation
Formation of granulomas (giant cells with central necrosis surrounded by plasma cells, lymphocytes, and dendritic cells) primarily in lungs and upper airways
ANCA-activated neutrophils release proinflammatory cytokines, attracting more neutrophils to endothelium (blood vessel wall)
ANCA-activated neutrophils undergo firm adhesion to endothelium
ANCAs stimulate ↑ secretion of proteolytic enzymes and reactive oxygen species from neutrophils
Endothelial damage and tissue injury
Granulomatosis with polyangiitis (GPA)
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms with involvement of multiple organ systems
(see slide on clinical findings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com
Granulomatosis with polyangiitis: Clinical findings Inflammation-mediated endothelial damage and granuloma formation
(see slide on pathogenesis)
Granulomatosis with polyangiitis (GPA)
Author:
Oswald Chen
Reviewers:
Ben Campbell
*Liam Martin
* MD at time of publication
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms
Fever, unintentional weight loss, night sweats, arthralgias
Skin involvement
Inflammation of cutaneous vessels
Systemic inflammation obstructing blood flow, with granulomatous lesions primarily in upper airways and lungs
Ear, nose, and throat involvement
↑ C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) (markers of inflammation)
Necrotizing granulomas on biopsy of affected tissue
Positive PR3-ANCA/c-ANCA blood test (antibodies present in ~90% of patients, described in GPA Pathogenesis slide)
Renal involvement
Inflammation of renal vessels
Rupture of basement membrane (layer that filters blood from glomerular capillaries into Bowman’s capsule)
Pauci-immune glomerulonephritis (see Nephritic Syndrome slide)
Rapidly progressive glomerulonephritis
Eye involvement
Inflammation of ocular tissue
Conjunctivitis
Scleritis/ episcleritis (painful red eye)
Lower respiratory tract involvement
Inflammation of pulmonary vessels
Vessel occlusion and ischemia
Skin necrosis
Vessels burst and blood pools under skin
Round and retiform (net- like) palpable purpura of lower extremities
Granulomatous destruction of nasal cartilage
Collapse of nasal bridge
Saddle nose deformity
Inflammation of paranasal sinus and nasal cavity vessels
↓ Perfusion of lungs
Dyspnea
Damage to interstitial capillaries
Hemoptysis
Diffuse alveolar hemorrhage
Rhinitis/ sinusitis
Granulomatous obstruction of eustachian tube
Otitis media (see Otitis Media slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com")
Granulomatosis with polyangiitis: Clinical findings

Granulomatosis with polyangiitis (GPA)
Author:
Oswald Chen
Reviewers:
Ben Campbell
*Liam Martin
* MD at time of publication
ANCA-associated vasculitis affecting medium and small-sized arteries, associated with necrotizing granulomas
Constitutional symptoms
Fever, unintentional weight loss, night sweats, arthralgias
Skin involvement
Inflammation of cutaneous vessels
Systemic inflammation obstructing blood flow, with granulomatous lesions primarily in upper airways and lungs
Ear, nose, and throat involvement
↑ C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) (markers of inflammation)
Necrotizing granulomas on biopsy of affected tissue
Positive PR3-ANCA/c-ANCA blood test (antibodies present in ~90% of patients, described in GPA Pathogenesis slide)
Renal involvement
Inflammation of renal vessels
Rupture of basement membrane (layer that filters blood from glomerular capillaries into Bowman’s capsule)
Pauci-immune glomerulonephritis (see Nephritic Syndrome slide)
Rapidly progressive glomerulonephritis
Eye involvement
Inflammation of ocular tissue
Conjunctivitis
Scleritis/ episcleritis (painful red eye)
Lower respiratory tract involvement
Inflammation of pulmonary vessels
Vessel occlusion and ischemia
Skin necrosis
Vessels burst and blood pools under skin
Round and retiform (net- like) palpable purpura of lower extremities
Granulomatous destruction of nasal cartilage
Collapse of nasal bridge
Saddle nose deformity
Inflammation of paranasal sinus and nasal cavity vessels
↓ Perfusion of lungs
Dyspnea
Damage to interstitial capillaries
Hemoptysis
Diffuse alveolar hemorrhage
Rhinitis/ sinusitis
Granulomatous obstruction of eustachian tube
Otitis media (see Otitis Media slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com")
Inhalational Injury

Acute hypoxemia
Loss of consciousness
Death
Upper airway injury (above vocal cords)
Cell lysis & necrosis
Local release of inflammatory substances
↑ Vascular permeability à edema of tissues in upper airway
Damage to lower respiratory tract cilia
↓ Mucus clearance from alveoli
Parenchymal injury
(delayed reaction dependent on severity of burn)
Alveolar epithelial and endothelial barrier irritation/damage
Inflammatory response
Carbon monoxide poisoning
Cyanide poisoning
Cyanide binds to mitochondrial cytochrome oxidase a3
CO binds more strongly to hemoglobin than O2
↑ Carboxyhemoglobin in blood, ↓ free hemoglobin available to bind O2 in the lungs
↑ Affinity for O2 on remaining binding sites in hemoglobin (i.e. hemoglobin binds O2 more strongly and is slow to release it)
↓ O2 delivered to tissues
Inhibition of cytochrome c oxidase
Mucous obstructs airways
Air retained
distal to the obstruction is resorbed from nonventilated alveoli
Regions without gas collapse i.e atelectasis
↑ Risk of infection
↓ Mitochondrial respiratory chain function
Impaired oxidative phosphorylation & cellular energy production
Cellular dysfunction in high metabolic tissues
Nitric oxide acts as a vasodilator in alveolar arterioles
Loss of hypoxic vasoconstriction (constriction of arterioles in alveoli due to ↓ O2)
Reactive inflammation & bronchoconstriction
Stridor
Complete airway obstruction
↑ Vascular permeability leading to fluid leakage into interstitium and alveoli
Blood flow to poorly ventilated alveoli is maintained
Ventilation/perfusion (V/Q) mismatch (regions of lung not effectively ventilated despite being well perfused by blood)
Acute Respiratory Distress Syndrome See ARDS Pathogenesis slide
Hypoxemia
Lower airway edema
Wheezing Coughing
Impaired brain function
Muscle weakness
Impaired heart function
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published November 10, 2019; Updated on February 12, 2023 on www.thecalgaryguide.com")
Large Bowel Obstruction: Findings on Abdominal X-ray
 and cecal or sigmoid volvulus (11-15%)
Obstruction from mechanical causes such as physical blockade of bowel lumen or twisting of the large bowel
Bowel Obstruction
*See Mechanical Bowel Obstruction and Ileus: Pathogenesis and clinical findings
Large bowel contents cannot pass the obstructionàgas buildup in colon from swallowed air, bacterial fermentation, CO2 from acid + bicarbonate reaction
Colon intraluminal pressure overcomes venous and lymphatic pressure
Impaired venous outflowàbowel wall edema/thickening
↑ Vascular resistance eventually impedes arterial inflowàbowel wall ischemia
Ischemia can progress to bowel infarction and necrosis
Large bowel loops are anatomically peripheral to the small bowel
Evacuation of gas and water reabsorption distal to obstruction
If ileocecal (IC) valve incompetent or sufficient pressure buildup in large bowel can overcome IC valve
↑ intraluminal pressure
Gas dissects into
bowel wall from mucosal disruption
Pneumatosis coli (air within bowel wall)
Bowel wall perforation (especially when cecum diameter > 10-12cm)
Dilated large bowel loops located peripherally (highlighted yellow)
Collapsed distal colon (few or no air-fluid levels in the large bowel as water is reabsorbed)
Small bowel dilatation (> 3 cm)
Colonic dilatation (> 6 cm)
Cecum dilatation (> 9 cm)
Haustra (anatomical folds of the large bowel) become visible as it is distended
Pneumoperitoneum (sub-diaphragmatic air on erect chest x-ray)
Release of gas into peritoneum
PA
Radiopaedia, rID:17957
PA
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 16, 2023 on www.thecalgaryguide.com")
Central Retinal Vein Occlusion

↓ Anticoagulation (e.g., Protein C or S def) and/or ↑ coagulation (e.g., malignancy, Polycythemia Vera)
Non-ischemic (perfused) CRVO
Glaucoma
(a disease characterized by ↑ intraocular pressure)
Optic disc drusen
(calcified nodules located within the optic disk – the most anterior part of the optic nerve)
Diabetes
Dyslipidemia
Hypertension
Vasculitis
(inflammation of blood vessels; e.g., sarcoid, Systemic Lupus Erythematosus)
Endothelial damage
Pupillary responses do not vary between both eyes when a light is shone in one eye at a time
Relative afferent pupillary defect (RAPD) mild or absent
Lost vascular wall integrity
Normal retinal electrical response to a light stimuli
Normal
electro- retinography (ERG) with b- wave >60%
Few scattered Intra-retinal hemorrhages
↓ In retinal electrical response to a light stimuli
Pupils respond differently to a light stimulus shone in one eye at a time
Severe ↓ in visual acuity (Snellen acuity of <20/400)
Visual field deficits
↓ b-wave amplitude (<60%) on ERG
RAPD present
↑ Pressure compromises retinal vein outflow
Central retinal atherosclerosis (build-up of fat & cholesterol plaque in arteries) & hardening
Atherosclerotic changes in the central retinal artery compress the central retinal vein (since they are both held together in region of the optic disc)
Venous stasis (stagnation of blood flow) ↑ Likelihood of thrombus formation
Central Retinal Vein Occlusion (CRVO)
A common retinal vascular disease characterized by blockage of the main vein that drains blood from the retina
CRVO classified based on the degree of perfusion (as seen through retinal angiography)
Ischemic (nonperfused) CRVO
↑ Intraluminal venous pressure
Dilated tortuous retinal veins
Normal visual fields
Vascular wall integrity lost
Four-quadrant hemorrhages described as “blood and thunder” on fundus exam
Obstruction due to thrombus
↓ Retinal capillary perfusion causes ischemia
Hypoxia in the retinal tissues
↑ Release of vascular endothelial growth factor to revascularize diseased tissue & overcome hypoxic conditions
Angiogenesis (formation of new blood vessels)
Intraretinal infarcts
“Cotton wool spots” on fundus exam
Venous capillary fluid/protein leakage
Mild retina, macula and disc edema
Moderate ↓in visual acuity often (Snellen acuity >20/400)
New vessel proliferation can occur in the anterior chamber of the eye
This change can block the outflow path of the aqueous humor in the eye
Neovascular glaucoma
Neovascular vessels are structurally different in comparison to regular retinal vasculature
Neovascular vessels are more fragile
↑ Likelihood of rupture Vitreous hemorrhage
Neovascular vessels lack tight junctions
↑ Fluid leakage
Retina, macula and disc edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First Published June 28, 2017, updated March 4, 2023 on www.thecalgaryguide.com")
Benzodiazepine Mechanism of Action
 receptor in vascular smooth muscle and the central nervous system (CNS)
APs inhibited in
vascular smooth muscle
Vascular smooth muscle relaxes
Vasodilation ↓ Blood pressure
Authors: Victoria Silva Travis Novak Reviewers: Billy Sun Mao Ding Melinda Davis* *MD at time of publication
↑ Frequency of chloride channel opening
Hyperpolarization of nerve membrane
Action potential (AP) inhibited
APs inhibited in the
medulla oblongata
(the respiratory center)
↓ Respiratory drive: the body fails to ↑ depth and rate of respirations when arterial CO2 ↑
General CNS inhibition
Anti-convulsion
(Seizures are caused by a burst of uncontrollable, electrical activity in the brain)
APs inhibited in the thalamus and hypothalamus (play a role in memory)
APs inhibited in the limbic system (the behavioral and emotional response centers in the brain)
Hypotension
↓ Cerebral blood flow
↓CO2 diffusion from arterial blood to alveoli
↓O2 diffusion from alveoli to arterial blood
Pharyngeal muscle relaxation
↑ Arterial CO2
↓ Arterial O2
Airway obstruction
Amnesia
↑ PaCO2
↓ PaO2
↓ Anxiety
Anxiolysis Hypercapnia
Hypoxemia
In high doses:
Depression of arousal and loss of consciousness
Induction of general anesthesia
(No analgesic effect)
↓ Intracranial pressure Benzodiazepine reversal:
Temporary cessation of breathing
Apnea
Flumazenil competitively binds to GABAA
Flumazenil reverses the binding of benzodiazepine to GABAA
↓ Frequency of chloride channel opening
Depolarization of nerve membrane
Benzodiazepine reversal
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 09, 2018, updated April 25, 2023 on www.thecalgaryguide.com")
diverticulosis-vs-diverticulitis-distinguishing-features
 contributing to reduced gut motility
↑Intraluminal pressure in the colon
Herniation of colonic mucosa and submucosa through circular muscle at points of weakness to form outpouchings
Diverticulosis
Presence of outpouchings in the colon (diverticuli)
Note: In Western populations, most diverticulosis is left-sided, whereas in Asian populations, these outpouchings are more often right-sided.
Mucosal abrasion or micro-perforation by ↑ intraluminal pressure or dense food particles
Bacterial overgrowth,
dysbiosis and passage into the lamina propria
Feces collects in diverticuli
Gut bacteria metabolize undigested material and produce gas
Stretching of colon Bloating wall irritates and
visceral afferent flatulence nerves
Episodic abdominal discomfort and cramping
Blood vessels in
the mucosa and submucosa (vasa recta) are stretched over the diverticuli, and may rupture from ↑ pressure
Diverticular bleed
Painless hematochezia (passage of fresh blood from the rectum)
Inflammatory cytokines activate clotting factors
Clotting of blood in vessels supplying diverticula
Inflammatory cytokine release (IL-6, TNF-α)
Cytokines enter systemic circulation
Edema in the bowel wall
Irritation of adjacent parietal peritoneum and somatic nerves
Left lower quadrant (LLQ) pain, guarding
Small abrasions are walled off by pericolic fat and mesentery
↑WBC
Fever
Inflammation may spread to nearby organs, leading to ulceration and abnormal connections between organs
Pericolic abscess
No hematochezia
Local ischemia and focal necrosis resulting in loss of integrity of the bowel wall
Perforation
Generalized peritonitis
Colonic obstruction (rare)
Fistulae (rare): i.e. colovesical, coloenteric
Stricture/fibros is formation with healing
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 12, 2016; Updated July 30, 2023 on www.thecalgaryguide.com")
Anesthetic Considerations for Obese Patients

Pre-oxygenate to ↑ oxygen reserve during intubation
Avoid supine positioning, in place of alternate positioning (i.e., reverse trendelenburg)
Lung-protective ventilation (↓ tidal volume, optimize oxygen levels, positive end
expiratory pressure & recruitment maneuvers)
Pre-operative fasting, gastric ultrasound to assess volume
Rapid sequence induction to reduce aspiration risk
Adjust drug dosages based on individual recommendations to account for altered distribution, metabolism & clearance
Excess body fat on chest wall
Excess intra- abdominal fat
↑ Gastric volume
Excess body fat
↑ Circulating blood volume
Obesity- related restrictive lung disease
↑ Load compressing chest wall
BMI
≥30
kg/m2
Note: effects vary with the severity of obesity
↑ Pressure on diaphragm and lungs
↓ Outward chest wall force
↑ Abdominal pressure
↑ Fat acts as a reservoir for lipophilic drugs
↑ Fat storage in hepatocytes
↑ Cardiac output
↑ Pressure on gastric contents
↑ Distribution half-life of lipophilic drugs
↑ Volume of distribution for lipophilic drugs
↑ Hepatic cytochrome transcription
↑ Glomerular filtration rate and hepatic blood flow
Authors: Brianna Rosgen
Reviewers: Kayleigh Yang
Ran Marissa Zhang
Karl Darcus*
* MD at time of publication
Legend:
Pathophysiology
Mechanism
Goal
Anesthetic Intervention
Published Nov 8, 2023 on www.thecalgaryguide.com")
Death Cardiovascular Respiratory and Neurologic Mechanisms

Hypoxemia (Type I Respiratory Failure): low dissolved oxygen in blood (PaO2)
Lungs can’t oxygenate blood fast enough
Lungs can’t rid blood of CO2 fast enough
Hypercapnia / hypercarbia (Type II Respiratory Failure): elevated dissolved CO2 in blood (PaCO2)
Cerebral vasodilation
Toxins: e.g. cyanide, pesticides, arsenic Severe anemia
Distributive problems:
Systemic inflammation (sepsis, anaphylaxis, pancreatitis), adrenal insufficiency, vasodilatory drugs
Obstructive problems: Cardiac tamponade*, tension pneumothorax* or massive pulmonary embolism*
Hypovolemic* problems (low blood volume): Hemorrhage, dehydration, widespread skin disruption or burns
Cardiac valve dysfunction
Myocardial infarction* or cardiomyopathy
Cardiac arrhythmia or heart block
Disturbed electrical activity in cardiomyocytes
Peripheral metabolic disturbances
Hypokalemia*, Hyperkalemia* Acidosis* (including renal failure) Hypothermia*
Toxins* (e.g. cocaine, beta blockers, tricyclics) Severe thyroid derangement
Inappropriate systemic vasodilation
Adjacent forces impair heart filling
Low cardiac preload
Low stroke volume (SV; depends on valves, contractility, preload)
Decreased systemic vascular resistance (SVR)
Low blood pressure (BP = CO x SVR)
Decreased cardiac output (CO = SV x HR)
Disseminated intravascular coagulationàwidespread thrombi that occlude blood flow (also causes hemorrhage, see relevant box at left)
Methemoglobinemia: some hemoglobin gets stuck in a state that can’t carry O2
Hemoglobin has reduced capacity to carry or release O2
Drugs: e.g. dapsone, nitrates
Carbon monoxide poisoning
Circulatory collapse / shock: inadequate perfusion of tissue with blood
Respiratory collapse: blood has insufficient useable O2 content
Ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT)
Hypoxia*: inadequate O2 delivery or utilization in tissues
Hypoxia creates metabolic disturbances that impair cardiac cells. Alternatively, any of the preceding conditions marked with (*) can directly trigger cardiac arrest first
Pulseless Electrical Activity (PEA): organized activity on ECG with no cardiac output (can be preceded or mimicked by pseudo-PEA, in which there is still some output on ultrasound)
Low atmospheric pressure or oxygen content Severe lung disease
Asthma, COPD, interstitial lung disease, congestive heart failure, pulmonary hypertension, pulmonary embolism, lung collapse / atelectasis
Acute respiratory distress syndrome
Pneumonia, aspiration pneumonitis, inhalational injury, systemic inflammation, drowning
Severe hypoventilation
Respiratory fatigue, advanced COPD, chest wall disorders, neuromuscular disorders, upper airway obstruction, toxins (e.g. opioids, botulism)
Can degenerate at any time
Asystole: no cardiac electrical activity or output
Death
Respiratory arrest: cessation of breathing
Inability to protect airway
Decreased level of consciousness
Note
This is a broad overview of the many scenarios that can result in death. For detailed explanations of the various disease mechanisms, refer to the corresponding slides.
* = reversible causes of cardiac arrest (Hs and Ts)
Author:
Ben Campbell
Reviewers:
Yan Yu*
Huma Ali*
* MD at time of publication
Bradycardia
(low heart rate, HR)
Unopposed parasympathetic stimulation of heart (can also cause vasodilation, see Distributive problems)
Disruption of spinal cord sympathetic control
Injury to cervical or upper thoracic spinal cord
Irreversible cessation of cardiac, respiratory, and brain function
Prolonged seizure initially causes increased cardiovascular activity, until the system fatigues
Disruption of respiratory control center in medulla
Expanding skull contents squeeze brainstem (herniation)
Increased intracranial pressure
Edema from intracranial hemorrhage, trauma, brain mass
Edema, inflammation, hypoxia and/or metabolic derangements cause diffuse neuron dysfunction
Central nervous system infection
Dementia, particularly with delirium
Massive ischemic stroke
Seizure
activity prevents or alters breathing
Metabolic disturbances that affect the central nervous system Hypoglycemia Hypocalcemia, hypercalcemia Hyponatremia, hypernatremia Uremia
Acute liver failure (hyperNH4) Many drugs / toxins Withdrawal (e.g. EtOH)
Status epilepticus
Brainstem lesion (e.g. stroke, neoplasm, inflammatory)
Nervous System Insult
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 11, 2023 on www.thecalgaryguide.com
Respiratory System Insult
Cardiovascular System Insult Cardiogenic problems")
Mechanical Ventilation mechanisms of action and complications
 when they cannot breathe on their own.
Invasive: Delivery of positive pressure to the lungs via endotracheal or tracheostomy tube
Mechanical ventilation
Pressure support ventilation (PSV): Set inspiratory pressure & flow. Patient initiates all breaths unassisted
Non-invasive: Delivery of oxygen into the lungs via positive pressure through the mouth
No endotracheal or tracheostomy tube
Assist/control ventilation (AC): Set respiratory rate & tidal volume (amount of air delivered to the lungs with each breath). Patient can trigger additional assisted breaths
Synchronized intermittent mandatory ventilation (SIMV): Set tidal volume & respiratory rate. Patient can trigger additional unassisted breaths
02 mask delivery
Continuous positive airway pressure (CPAP)
Provides continuous positive ventilatory pressure
Bilevel positive airway pressure (BIPAP)
Provides positive pressure with two different pressure levels for inhalation and exhalation
↑ Swallow non- inspiratory flow
Aspiration
Acute rise in airway pressure
Barotrauma
Patient- triggered breath
Ventilator senses negative pressure from inflation of the lungs
Time-triggered breath
Respiratory rate set at x breaths per min
Patient-triggered breath
Ventilator senses negative pressure from inflation of the lungs
Tidal volume determined by patient’s strength & lung compliance
Time-triggered breath
Respiratory rate set at x breaths per min
Delivery of set tidal volume, inspiratory flow rate & pattern
Complete patient- triggered breaths
Ventilator senses negative pressure from inflation of the lungs
Breathes assisted by set inspiratory pressure
Inspiratory flow drops below set inhalational negative pressure threshold
Pressure support terminates as exhalation cycle begins
Combined with SIMV
Inspiratory pressure added to patient triggered breaths
Patient can overcome resistance of the endotracheal tube or ↑ volume of spontaneous breathes
Delivery of set tidal volume, inspiratory flow rate & pattern
Airways remain open & clear of obstruction
Forced air into nasal passages
Nose bleeds (epistaxis)
Maximum tidal volume reached
Exhale valve opens
Patient exhales actively or passively until set end expiratory pressure in the lungs is reached (PEEP) to prevent alveolar collapse
Patient exhales until PEEP reached
Patient achieves optimal ventilation throughout respiratory cycles
Mouth breathing
Dry mouth
(xerostomia)
Increased work of breathing & muscle fatigue
Prolonged weaning & extubation
Breath stacking
↑ Volume and pressure in lungs Lung tissue injury (barotrauma)
Microorganisms colonize artificial airway
Ventilator associated pneumonia if ventilation >48 hrs
Tachypnea
↓ CO2in circulation Respiratory alkalosis
Legend:
Pathophysiology
Mechanism
Sign/symptom/lab finding
Complications
Published Nov 25, 2023 on www.thecalgaryguide.com")
Anesthetic Considerations One Lung Ventilation
 with dependent lung ventilated
Shunt: Non- dependent lung unventilated
Perfusion but no ventilation to collapsed lung
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch causes ↑ hypoxemia
Increase FiO2 to 1 to maintain SpO2 ≥ 90%
Increased FiO2 can allow for toleration of shunt
Optimize cardiac output and shunt fraction to maximize PaO2
Author:
Aly Valji
Reviewers:
Jasleen Brar
Ryden Armstrong*
* MD at time of publication
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Double lumen tube (gold standard)
Endotracheal tube (ETT) with two lumens (bronchial and tracheal)
Insert longer side to a mainstem bronchus, shorter side ends in distal trachea
Absolute Indications
Isolation of healthy from contaminated lung (unilateral infection, hemorrhage)
Control unilateral disruption of ventilation (bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Airway Technique
Anesthetic Technique
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Intraabdominal contents push up on diaphragm
↓ Functional residual capacity (FRC)
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize
Altered gravitational forces on thorax
↓ Compliance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent lung. ↑ Ventilation to nondependent lung (prior to lung isolation)
Collapse of nondependent lung using lung isolation causes ↓ ventilation to this lung
Optimize tidal volume (6-8 mL/kg), respiratory rate (maintain PaCO2 35-40 mmHg), PEEP (5-10 cm H2O) based on clinical picture
Univent tube
Single lumen ETT with movable endobronchial blocker in wall
Blocker steered after intubation into a mainstem bronchus with fiberoptic bronchoscope
Endotracheal tube in mainstem bronchus
Single lumen ETT pushed into a mainstem bronchus
Bronchial blocker
Shaft with an inflatable balloon on distal end
Inserted through single lumen ETT into a mainstem bronchus, after intubation
positive end- expiratory pressure (PEEP) of 5-10 cm H2O
Recruitment of dependent, atelectatic lung with positive pressure
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Cuff inflated in a mainstem bronchus to isolate respective lung. Placement should be verified using fiberoptic bronchoscope if possible after positioning
↓ Atelectasis and ↑ FRC
↓ Hypoxemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Management
Published December 5, 2023 on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Shunt: Non- dependent lung unventilated
Perfusion but no ventilation to collapsed lung
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to 1 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Author:
Aly Valji
Reviewers:
Jasleen Brar
Dr. Armstrong*
* MD at time of publication
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Double lumen tube (DLT)
Two endotracheal tubes (ETT) bonded together
Insert longer side to a mainstem bronchus, shorter side ends in distal trachea
Absolute Indications
Isolation of healthy from contaminated lung (unilateral infection, hemorrhage)
Control unilateral disruption of ventilation (bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Airway Technique
Anesthetic Technique
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Intraabdominal contents push up on diaphragm
↓ Functional residual capacity (FRC)
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize
Altered gravitational forces on thorax
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume (6-8 mL/kg), respiratory rate (maintain PaCO2 35-40 mmHg), PEEP (5-10 cm H2O) based on clinical picture
Univent tube
Single lumen ETT with movable endobronchial blocker in wall
Blocker steered after intubation into a mainstem bronchus with fiberoptic bronchoscope
Endotracheal tube in mainstem bronchus
Single lumen ETT pushed into a mainstem bronchus
Bronchial blocker
Shaft with an inflatable balloon on distal end
Inserted through single lumen ETT into a mainstem bronchus, after intubation
positive end- expiratory pressure (PEEP) of 5-10 cm H2O
Recruitment of dependent, atelectatic lung with positive pressure
Optimize
FiO
2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Cuff inflated in a mainstem bronchus to isolate respective lung. Placement should be verified using fiberoptic bronchoscope if possible after positioning
↓ Atelectasis and ↑ FRC
↓ Hypoxemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Management
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Relative indications
Surgical exposure for pulmonary resection, mediastinal, esophageal, vascular, thoracic spine surgery
Absolute Indications
Isolation of healthy from contaminated lung (Unilateral infection or hemorrhage)
Control unilateral disruption of ventilation (Bronchopleural fistula, unilateral bullae)
Video assisted thoracoscopic surgery
Unilateral lung lavage
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia
Altered gravitational forces on thorax
Shaft with an inflatable balloon on distal end. Inserted through a single lumen ETT after intubation into a mainstem bronchi
Single lumen ETT pushed into a mainstem bronchus
Optimize positive end-expiratory pressure (PEEP))
Recruitment of dependent, atelectatic lung with positive pressure
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
Bronchial blocker
Endotracheal tube in mainstem bronchus
Technique
Univent tube
Double lumen tube (DLT)
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O2 and ↓ N2)
Single lumen ETT with movable endobronchial blocker housed in wall of ETT. Blocker maneuvered after intubation into a mainstem bronchus
Two endotracheal tubes (ETT) bonded together. Longer side goes into a mainstem bronchus, shorter side ends in distal trachea
↓ Atelectasis and ↑ FRC
↓ V/Q mismatch
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO to 2
maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Comorbidity: Likely underlying pulmonary disease
Pre-operative evaluation
Pulmonary function testing
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Multidisciplinary determination of fitness for surgery
Pulmonary hemorrhage Whole lung lavage Unilateral infection Bronchopleural fistula
Isolation of affected lung from unaffected lung
Pulmonary resection
Mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Operative lung deflated to expose surgical site
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis if closing capacity > FRC
↑ Hypoxemia Optimize positive
Altered gravitational forces on thorax
Contraindications
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
Bilateral lung ventilation dependency
Hemodynamic instability
Severe hypoxia Severe COPD
Severe pulmonary hypertension
Potentially unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass
Known difficult airway
Risk of dislodging mass and inability to secure airway
Pursue more advanced airway techniques
end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
Optimize FiO2
↓ Absorptive atelectasis (from ↑ partial pressure O and ↓ N )
2
2
↓ Atelectasis and ↑ FRC
Post-operative pain management
Thoracotomy or VATS procedure causing ↑ pain along thoracic dermatomes
Epidural
Paravertebral block
Anesthetic injected into epidural space
Anesthetic injected into paravertebral spaces
Bilateral spinal nerve blockade below desired spinal level
Ipsilateral spinal nerve and sympathetic chain blockade in thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Jasleen Brar Name* * MD at time of publication
Non-dependent lung unventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
Right to left intrapulmonary shunt with some perfusion to non- dependent lung
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
Indications
Anesthetic
General anesthetic with neuromuscular blockade
↓ Inspiratory muscle tone
Comorbidity: Likely underlying pulmonary disease
Pre-operative evaluation
Pulmonary function testing
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Multidisciplinary determination of fitness for surgery
Anesthetic injected into epidural space
Anesthetic injected into paravertebral spaces
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
Pulmonary hemorrhage Whole lung lavage Unilateral infection Bronchopleural fistula
Isolation of affected lung and unaffected lung
Pulmonary resection
Mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Operative lung deflated to expose surgical site
Intraabdominal contents push up on diaphragm
↓ FRC
↑ Atelectasis ↑ Hypoxemia
Optimize
positive end- expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
↓ Atelectasis and ↑ FRC
Altered gravitational forces on thorax
Contraindications
↑ Elastance of dependent lung
↑ Airway pressure required
↑ Risk of lung barotrauma due to ↑ pressure
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
↑ Perfusion to dependent, ventilated lung
↓ Ventilation- perfusion (V/Q) mismatch
↓ Hypoxemia
Bilateral lung ventilation dependency
Hemodynamically unstable
Severe hypoxia Severe COPD
Severe pulmonary hypertension
Unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass
Known difficult airway
Risk of dislodging mass and inability to secure airway
Pursue more advanced airway techniques
Post-operative pain management
Thoracotomy or VATS procedure causing ↑ pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired spinal level
Ipsilateral spinal nerve and sympathetic chain blockade in thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation Mechanical separation of the lungs to allow for individualized ventilation of only one lung
Author:
Aly Valji Reviewers: Name* * MD at time of publication
Indication
Contraindications
Comorbidity: Likely underlying pulmonary disease
Positioning: Lateral decubitus position (patient on their side) with dependent lung ventilated
General anesthetic with neuromuscular blockade
Post-operative pain management
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Operative lung deflated to expose surgical site
Isolation of affected lung and unaffected lung
Dependency on bilateral lung ventilation, hemodynamically unstable, severe hypoxia, severe COPD, or severe pulmonary hypertension
Unable to tolerate one lung ventilation
Intraluminal airway obstruction/mass or known difficult Pursue more advanced
Risk of dislodging mass and inability to secure airway
Multidisciplinary determination of fitness for surgery
airway
Pulmonary function testing
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
airway techniques
Overall clinical picture, forced expiratory volume (FEV1), and diffusion capacity (DLCO)
Pre-operative evaluation
Non- dependent lung not ventilated
Altered gravitational forces on thorax
Intraabdominal contents push up on diaphragm
↓ Inspiratory muscle tone
Likely procedure is thoracotomy or VATS causing ↑ pain along thoracic dermatomes
Right to left intrapulmonary shunt with some perfusion to non- dependent lung still present
V/Q mismatch from shunt causes ↑ hypoxemia
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for shunt to non- dependent lung
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP based on clinical picture
↓ Atelectasis and ↑ FRC
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
↓ Functional residual capacity (FRC)
↓ Ventilation-perfusion (V/Q) mismatch
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma due to ↑ pressure
Intervention:
Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung with positive pressure
Epidural
Paravertebral block
Anesthetic injected into epidural space
Bilateral spinal nerve blockade below desired spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in thoracic paravertebral spaces dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic Considerations: One-lung ventilation
Author:
Aly Valji Reviewers: Name* * MD at time of publication
One lung ventilation: mechanical separation of the lungs to allow for individualized ventilation of only one lung
Indication
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Exposure of surgical site by deflation of operative lung
Isolation of affected lung and unaffected lung
Dependency on bilateral lung ventilation, Contraindications hemodynamically unstable, severe hypoxia, severe
COPD, or severe pulmonary hypertension
Intraluminal airway obstruction/mass or known difficult airway
Pursue more advanced airway techniques
Unable to tolerate one lung ventilation
Risk of dislodging mass and inability to secure airway
Likely underlying Pre-operative Pulmonary pulmonary disease evaluation function testing
Overall clinical picture, forced expiratory Determination of volume (FEV1), and diffusion capacity (DLCO) fitness for surgery
Right to left intrapulmonary shunt as some perfusion to non- dependent lung is still present
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
Non- dependent lung not ventilated
Hypoxic vasoconstriction decreases but does not stop perfusion to non- dependent lung
V/Q mismatch from shunt increases hypoxemia
Intervention:
Increase FiO2 to maintain SpO2 ≥ 90%
Vasodilation of dependent lung vasculature to compensate for non-dependent lung
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP
↓ Atelectasis and ↑ FRC
Positioning: Lateral position with dependent lung ventilated
Altered gravitational forces on thorax
↓ Ventilation-perfusion (V/Q) mismatch
General anesthetic with neuromuscular blockade
Intraabdominal contents push up on diaphragm
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma
Intervention: Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent, atelectatic lung from PEEP
↓ Inspiratory muscle tone
↓ Functional residual capacity (FRC)
Post- operative pain management
Thoracotomy or VATS causes pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired Anesthetic injected into epidural space spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in paravertebral spaces thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com
Anesthetic considerations: one-lung ventilation
Author:
Aly Valji Reviewers: Name* * MD at time of publication
One lung ventilation: mechanical separation of the lungs to allow for individualized ventilation of only one lung
Indication
Pulmonary resection, mediastinal, esophageal, vascular, thoracic spine, or cardiac valve surgery
Pulmonary hemorrhage, whole lung lavage, bronchopleural fistula, or unilateral infection
Exposure of surgical site by deflation of one lung
Isolation of one lung from other
Dependency on bilateral lung ventilation, Contraindications hemodynamically unstable, severe hypoxia, severe
COPD, or severe pulmonary hypertension
Intraluminal airway obstruction/mass or known difficult airway
Pursue more advanced airway techniques
Unable to tolerate one lung ventilation
Risk of dislodging mass and inability to secure airway
Pre-operative evaluation given likely Pulmonary Forced expiratory volume (FEV1) Determination of underlying pulmonary disease function testing Diffusion capacity (DLCO) fitness for surgery
Non- dependent lung not ventilated
Hypoxic vasoconstriction decreases but does not stop perfusion of non- dependent lung
Vasodilation of dependent lung pulmonary vasculature
Right to left intrapulmonary shunt causes V/Q mismatch
↑ Perfusion to dependent, ventilated lung
↑ Elastance of dependent lung
↓ FRC
↑ Hypoxemia
Intervention:
Increase FiO2 to maintain SpO2 ≥ 90%
↓ V/Q mismatch
↓ Hypoxemia
Intervention:
Optimize tidal volume, respiratory rate, PEEP
↓ Atelectasis and ↑ FRC
Positioning: Lateral decubitus with dependent lung ventilated
Altered gravitational forces on thorax
↓ Ventilation-perfusion (V/Q) mismatch
General anesthetic with neuromuscular blockade
Intraabdominal contents push up on diaphragm
↑ Airway pressure required
↑ Atelectasis ↑ Hypoxemia
↑ Risk of lung barotrauma
Intervention: Optimize positive end-expiratory pressure (PEEP)
Recruitment of dependent lung
↓ Inspiratory muscle tone
↓ Functional residual capacity (FRC)
Post- operative pain management
Thoracotomy or VATS causes pain along thoracic dermatomes
Epidural
Paravertebral block
Bilateral spinal nerve blockade below desired Anesthetic injected into epidural space spinal level
Anesthetic injected into Ipsilateral spinal nerve and sympathetic chain blockade in paravertebral spaces thoracic dermatomes
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complication/Intervention
Published MONTH, DAY, YEAR on www.thecalgaryguide.com")
Zenkers Diverticulum Pathogenesis and Clinical Findings
 resting pressure
Inadequate relaxation of the cricopharyngeal muscle of the UES during swallowing
Lack of synchronization between UES and hypopharynx during swallowing
Outflow obstruction in the esophagus
Increased intrabolus pressure with swallowing
Increase in hypopharyngeal pressure
Note: the pathogenesis of Zenker’s Diverticulum is multifactorial, but this mechanism is thought to be a significant contributor
Herniation of the esophagus at a weak point
between the inferior pharyngeal constrictor muscle and the cricopharyngeal muscle (Killian’s triangle)
Zenker’s Diverticulum
Acquired mucosal herniation between the horizontal and oblique fibers of the cricopharyngeus muscle
Inability of the the upper esophageal sphincter to completely open
Dysphagia
Extrinsic compression of the cervical esophagus by the diverticulum
Esophageal Obstruction
Diverticulum compresses recurrent laryngeal nerve
Impaired
innervation to
the intrinsic
muscles of
the larynx
and other
contributing
factors
False diverticulum retains food and saliva
Feeling of needing to clear throat
Palpable lump in the neck
Halitosis (bad smelling breath)
Secretions and food spontaneously empty into the bronchial tree
Splashing of the fluid that has accumulated in large diverticula
Cricoid Cartilage
Cricopharyngeal muscle of the UES
Thyroid Gland
Boyce’s sign (gurgling sound heard as air passes through the diverticulum)
Zenker’s Diverticulum
Weight loss and malnutrition
Aspiration
Cough reflex
Chronic cough
Regurgitation Hoarseness
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 25, 2023 on www.thecalgaryguide.com")
Bacterial Tracheitis

Children at higher risk due physiologic narrowing of airway
Recent upper respiratory viral infection
(often in Fall/Winter; respiratory virus season) Damage to airway mucosa
Activation of systemic inflammatory response
Inflammatory cytokines release into systemic circulation
↑ Thermo-regulatory set- point at the hypothalamus
↑ Work of breathing to adequately ventilate lungs
Respiratory distress (nasal flaring, grunting)
Activation of local inflammatory response
Results in thick mucopurulent secretions, ulcerations, and shedding of tracheal mucosa
Mucopurulent discharge
secretion of fluid contains mucus and pus
↑ Production of mucous results in more accumulation
Predisposition to bacterial infection
Bacterial pathogen invades trachea Ex: S. aureus (common), S. pyogenes, M. catarrhalis, or H. influenzae
Often high fever
Trachea is narrowed with purulent debris
Upper airway obstruction causes turbulent airstreams
Hoarse voice Tachypnea
Stridor
(with inhalation & exhalation; may be biphasic)
Tracheal tenderness
↓ Mucous clearance from the airways
Excess airway mucous triggers cough reflex
Cough
(may be barky)
↑ Use of accessory
respiratory muscles
(sternocleidomastoid and scalene muscles)
Toxic appearance (lethargy, cyanosis)
↓ Level of consciousness (due to hypoxia & hypercarbia)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 11, 2024 on www.thecalgaryguide.com")
Epiglottitis
, viral or fungal
Authors: Alisha Ebrahim Reviewers: Simran Sandhu Mao Ding Michelle J. Chen Danielle Nelson* * MD at time of publication
Infectious agent invades the bloodstream and/or the epithelial layer of the epiglottis, aryepiglottic folds and adjacent structures, allowing for spread
Non-infectious cause: Ingestion of toxin or foreign body, thermal injury, or trauma
The potential space between the squamous epithelial layer and the epiglottal cartilage fills with inflammatory cells such as neutrophils and eosinophils
Exudate of inflammatory cells spreads through the lymphatic and blood vessels in the lingual surface of the epiglottis and periepiglottic tissues
Fluid and inflammatory cells accumulate between the squamous epithelial layer and epiglottal cartilage
Swelling of the entire supraglottic larynx
Tripod/sniffing position (Anxious- looking and sitting with trunk leaning
forward, neck hyper-extended and chin pushed forward to maximize airway diameter)
Stridor (High-pitched sound that is produced by obstruction in the larynx or just below)
Stertor (Low-pitched noise created in the nose or the back of the throat)
Retraction of the intercostal and suprasternal muscles
Tachypnea (Rapid breathing)
Increased weight and mass of the epiglottis Epiglottis curls posteriorly and inferiorly
Ball-valve effect (Airflow obstructed during inspiration as epiglottis is pulled over airway but not during expiration as epiglottis moves back into position)
↓ Diameter of upper airway
Epiglottis obstructs the esophagus
Dysphagia (Difficulty swallowing)
Cyanosis (Blue tint to skin)
Turbulent inspiratory airflow Aspiration of oropharyngeal secretions
Hypoxemia (Low oxygen levels in blood)
↓ Air entry to lungs
Airway obstruction
↑ Work of breathing
Drooling Pain when swallowing
Muffled/”hot potato” voice
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 5, 2024 on www.thecalgaryguide.com")
Acute Otitis Externa Complications
: Complications
Acute Otitis Externa (AOE)
Authors: Charmaine Szalay-Anderson Vaneeza Moosa Reviewers: Shayan Hemmati Shahab Marzoughi Ben Campbell Justin Lui* * MD at time of publication
Spread to subcutaneous tissue
Chronic otitis externa (>6 weeks)
Chronic inflammation of the outer ear
Fibroblast activation for collagen and extracellular matrix components production for tissue repair
Excess accumulation of tissue
Ear canal fibrosis (thickening)
Ear canal stenosis (narrowing)
Damage/obstruction to ear canal structures with impaired fluid drainage & pressure buildup
Inflammation of the outer ear
Recurrent or non-resolving acute otitis externa Dissemination of infection
Spread to connective tissue and cartilage
Perichondritis (inflammation of ear cartilage)
Spread of Pseudomonas aeruginosa
in an immunocompromised host or due to antibiotic resistance
Rapid infectious spread through soft tissue to mastoid and/or temporal bone
Malignant (necrotizing) otitis externa *can be life threatening
Inflammation of connective tissue and bony structures
Spread to
tympanic membrane
Myringitis (inflammation of tympanic membrane)
Swelling and thinning of tissue
Tympanic membrane perforation (tear)
Immune reaction with inflammation
Dead white blood cell, bacteria & tissue debris accumulation in the ear canal
Pus formation with purulent otorrhea (discharge from ear)
Localized pus accumulation
Abscess
Ear canal blockage
Periauricular/ pinna (outer ear) cellulitis
Facial cellulitis
Erosion of temporal bone decreasing bony sound conduction
Permanent conductive hearing loss
Direct toxicity of pathogens to surrounding nerves
Cranial nerve (CN) VII (facial) palsy (+/- CN X, XI, XII)
Out-of- proportion primary otalgia (ear pain)
Sensation of fullness in the ear
Temporary hearing loss
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 4, 2022; updated Feb 7, 2024 on www.thecalgaryguide.com")
Angioedema Bradykinin Mediated
 & precursors (kininogen), triggered by ↑ systemic estrogen
Rheumatologic disorders & B- cell lymphoproliferative disease
Complement cascade activation results in ↑ C1 protease production
C1 esterase inhibitor is utilized to neutralize C1 protease, with its consumption exceeding its synthesis
Plasma cell proliferation (i.e., dyscrasia/ monoclonal gammopathy)
Immunoglobulin G antibodies act against C1 esterase inhibitor to render it non-functional
Genetic or spontaneous mutation in C1 esterase inhibitor gene
C1 esterase inhibitor deficiency
C1 esterase inhibitor dysfunction
Inhibition of angiotensin converting enzyme, dipeptidyl peptidase-4, or neprilysin induced metabolism of bradykinin
↓ Bradykinin (peptide hormone) degradation in plasma
Misfunctioning C1 esterase inhibiter is unable to inactivate bradykinin cascade members
↓ C1 esterase inhibiter results in inadequate inactivation of bradykinin cascade members
↑ Bradykinin protein production in plasma
Cutaneous Tissue
Mucosal Tissue
Epidermal layer
Dermal-Epidermal Junction
Dermal layer
Subcutaneous layer
Systemic bradykinin excess
Bradykinin-2 receptor binding on endothelial and vascular smooth muscle cells Hyperpermeability pathway activation, with the transcription of some signalling molecules taking hours Released pro-inflammatory mediators act on venules & arterioles in subcutaneous & submucosa tissues
Relaxation of vascular smooth muscle Dissociation of endothelial cell junctions
↑ Capillary blood flow ↑ Vascular permeability
↑ Plasma release into interstitial tissues (specific regions of the body hypothesized to be affected due to local differences in endothelial structure and its response to permeability inducing stimuli)
Dilation & ↑ permeability of vasculature results in fluid release into surrounding tissues
Mucosal Layer
Muscularis mucosae
Submucosal layer
Muscularis externa
Intestinal edema (Fluid buildup in Intestine tissues)
Intestinal swelling (↑ intra-abdominal pressure)
Laryngeal edema (Fluid buildup in larynx)
Swelling in larynx ↓ air flow into & out of lungs
Asphyxia (body is deprived of oxygen) Dyspnea (difficult in breathing)
Author: Aaron Varga Reviewers: Tracey Rice Sunawer Aujla Shahab Marzoughi Maharshi Gandhi Jori Hardin* Yan Yu* * MD at time of publication
Peripheral edema (Fluid buildup in extremities such as the hands, ankles, and feet)
Ascites, bowel obstruction, &/or hypovolemic shock
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 21, 2024 on www.thecalgaryguide.com")
Apnea of Prematurity
![Apnea of Prematurity: Pathogenesis, Signs & Symptoms, and Complications Physiologic immaturity from birth at < 37 weeks gestation
Authors: Akaya Blair Reviewers:
Dasha Mori Michelle J. Chen Danielle Nelson* * MD at time of publication
↓ Synaptic connection & poor myelination
Fetal brain areas responsible for breathing are poorly developed Immature neurologic respiratory function
Immature mechanical respiratory function
Poor hypopharyngeal muscle tone (soft upper airway helps with size and compliance of airway)
Nasal obstruction (e.g. anatomic and/or iatrogenic [suctioning, NG tubes])
Neonate is reliant on nose breathing
Airway is unable to remain open (patent)
Laryngeal/tracheal abnormalities (e.g. tracheomalacia, laryngeal edema, tracheal stenosis)
Anatomical narrowing leading to ↑ airway resistance
↑ Risk of mechanical airway obstruction
Disruption of central respiratory drive
↓ Sensitivity to increased CO2 in the ventral medulla oblongata
Disruption of peripheral respiratory reflex pathways
↓ Sensitivity to CO2 levels in peripheral carotid bodies and aortic bodies
Large head size forces neck into flexion when laying supine
Immature airway sensitive to collapse when in flexion
↑ Hypotonia (decreased muscle tone) in REM sleep
↓ Signaling to brainstem
Brainstem unable to mount appropriate ventilatory response to insufficient oxygen
Upper airway collapse
Apnea of prematurity
Respiratory pauses >20 sec or pauses <20 sec with bradycardia (<100 beats per minute), central cyanosis, and/or oxygen saturation <85% in neonates born at <37 weeks gestation and with no underlying disorders causing apnea. Most apneas in apnea of prematurity are central or mixed.
↓ Breathing rate
Bradycardia (<100 bpm)
↓ Oxygen to brain
Poor neurodevelopmental outcomes (e.g. cognitive function, brain adaptive potential and plasticity)
Hypoxemia (↓blood oxygen levels where SpO2 <85%)
↓ Oxygen and hemoglobin to mucous membranes (e.g. lips) & fingers and toes (periphery)
Central & peripheral cyanosis (bluish discoloration)
↓ Oxygen to retina
Abnormal growth of blood vessels in eyes
Retinopathy of prematurity (changes in visual acuity and possible blindness)
Death/impairment in cell function from lack of oxygen
↑ Risk of infant mortality
Imbalanced oxygen intake and CO2 output in lungs
Body transiently ↑ HR to unsuccessfully try to compensate for ↓ tissue oxygenation
Respiratory failure
Respiratory rate >60 ↓ Heart rate
↓ Blood pressure
Head bobbing Abdominal breathing
Skin mottling
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 21, 2024 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2024/03/Apnea-of-Prematurity.jpg "Apnea of Prematurity: Pathogenesis, Signs & Symptoms, and Complications Physiologic immaturity from birth at < 37 weeks gestation
Authors: Akaya Blair Reviewers:
Dasha Mori Michelle J. Chen Danielle Nelson* * MD at time of publication
↓ Synaptic connection & poor myelination
Fetal brain areas responsible for breathing are poorly developed Immature neurologic respiratory function
Immature mechanical respiratory function
Poor hypopharyngeal muscle tone (soft upper airway helps with size and compliance of airway)
Nasal obstruction (e.g. anatomic and/or iatrogenic [suctioning, NG tubes])
Neonate is reliant on nose breathing
Airway is unable to remain open (patent)
Laryngeal/tracheal abnormalities (e.g. tracheomalacia, laryngeal edema, tracheal stenosis)
Anatomical narrowing leading to ↑ airway resistance
↑ Risk of mechanical airway obstruction
Disruption of central respiratory drive
↓ Sensitivity to increased CO2 in the ventral medulla oblongata
Disruption of peripheral respiratory reflex pathways
↓ Sensitivity to CO2 levels in peripheral carotid bodies and aortic bodies
Large head size forces neck into flexion when laying supine
Immature airway sensitive to collapse when in flexion
↑ Hypotonia (decreased muscle tone) in REM sleep
↓ Signaling to brainstem
Brainstem unable to mount appropriate ventilatory response to insufficient oxygen
Upper airway collapse
Apnea of prematurity
Respiratory pauses >20 sec or pauses <20 sec with bradycardia (<100 beats per minute), central cyanosis, and/or oxygen saturation <85% in neonates born at <37 weeks gestation and with no underlying disorders causing apnea. Most apneas in apnea of prematurity are central or mixed.
↓ Breathing rate
Bradycardia (<100 bpm)
↓ Oxygen to brain
Poor neurodevelopmental outcomes (e.g. cognitive function, brain adaptive potential and plasticity)
Hypoxemia (↓blood oxygen levels where SpO2 <85%)
↓ Oxygen and hemoglobin to mucous membranes (e.g. lips) & fingers and toes (periphery)
Central & peripheral cyanosis (bluish discoloration)
↓ Oxygen to retina
Abnormal growth of blood vessels in eyes
Retinopathy of prematurity (changes in visual acuity and possible blindness)
Death/impairment in cell function from lack of oxygen
↑ Risk of infant mortality
Imbalanced oxygen intake and CO2 output in lungs
Body transiently ↑ HR to unsuccessfully try to compensate for ↓ tissue oxygenation
Respiratory failure
Respiratory rate >60 ↓ Heart rate
↓ Blood pressure
Head bobbing Abdominal breathing
Skin mottling
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 21, 2024 on www.thecalgaryguide.com")
Post-Renal Acute Kidney Injury AKI
: Pathogenesis and clinical findings
Blood clot or cellular debris
Foreign body
Neurogenic bladder
Obstruction intrinsic to urine excretion system
Nephrolithiasis (kidney stones)
Anatomical defect(s)
Intra- abdominal adhesions
Retroperitoneal fibrosis (scar-like tissue)
Benign or malignant masses
Prostate cancer
Benign prostatic hyperplasia
↓ Urine flow across point of obstruction Obstruction extrinsic to urine excretion system
Urine buildup distends urine collecting system (hydronephrosis)
Compression of renal vasculature due to mass effect
↑ Volume/pressure proximal to obstruction
↑ Intratubular pressure
↓ Pressure gradient between glomerular afferent arteriole and Bowman’s space
Casts occlude tubules
↓ Filtration of plasma into nephrons
↓ Glomerular Filtration Rate (GFR)
Obstruction is relieved ↓ Intratubular pressure Rapid GFR ↑
Rapid diuresis of fluid and electrolytes
Dilated pelvicalyceal system on ultrasound
↓ Urine output
↓ Venous drainage
and arterial supply
Local ischemia and inflammation of kidney
Impaired resorption, excretion, and fine tuning by tubules
Acute Tubular Necrosis (ATN) with granular casts
↓ Urine output
↓ Clearance of free water and solutes
↑ Intravascular volume
↑ Serum creatinine
↓ Medullary solute concentration, ischemia, ↓ response of collecting ducts to antidiuretic hormone
Lasts > 24hrs
Post-obstructive diuresis causes hypovolemia and electrolyte derangements
Authors: David Campbell, Matthew Hobart Reviewers: Raafi Ali, Luiza Radu Huneza Nadeem, Marissa Zhang, Julian Midgley* * MD at time of publication
Resolves < 24hrs in euvolemia
Physiologic post- obstructive diuresis
↑ Na+ and Cl- delivery to distal convoluted tubule is sensed by macula densa
Secretion of adenosine by macula densa
Adenosine constricts afferent arterioles
↓ GFR
↓ Renal clearance of drugs and waste products
↑ Venous hydrostatic pressure
↑ Volume in arterial system overwhelms pressure regulation mechanisms
Hypertension
Fluid extravasation from veins and capillaries
Generalized Edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Mar 25, 2024 on www.thecalgaryguide.com")
Overview of Ischemic Heart Disease
: Pathogenesis of the various types of IHD
Authors:
Sean Spence Vaneeza Moosa Reviewers: Tristan Jones Jason Baserman Yan Yu
Michelle J. Chen Frank Spence* * MD at time of publication
↑ Serum low-density lipoprotein (LDL)
↑ Availability of lipids that deposit in arterial wall
↓ Serum high-density lipoprotein (HDL)
↓ LDL removal from coronary artery walls (transport of LDL to liver is impaired)
Atherosclerosis
Conditions predisposing to vessel wall endothelial cell dysfunction (e.g. metabolic syndrome, smoking, hypertension, physical inactivity)
Vessel wall vulnerable to infiltration by LDL and immune cells
Arterial wall degeneration, characterized by fat deposition (atheromatous plaque) in and fibrosis of the inner layer of arteries
Stable atheromatous plaque in coronary arteries
Fibromuscular cap (formed by smooth muscle cells) overlying fatty plaque contents remains intact & plaque contents are not released into vessel lumen
Plaque serves as a fixed lumenal obstruction to blood flow
If vessel stenosis (narrowing) is significant (≥70%) myocardial oxygen demand starts to exceed supply (especially with exertion)
Heart experiences a predictable & transient reduction in blood flow (myocardial ischemia)
Unstable atheromatous plaque in coronary arteries
The fibromuscular cap overlying fatty plaque ruptures
Thrombogenic plaque contents (especially tissue factor) are exposed to the coagulation factors in the vessel lumen
Activation of platelets & the clotting cascade at the site of rupture
Thrombus forms over already partially occlusive plaque and further partially or completely occludes lumen
↓ Perfusion (blood flow) of myocardium
Cardiomyocytes experience a transient decrease in blood flow (transient ischemia)
Unstable Angina
Cardiomyocytes experience death (infarction)
Myocardial Infarction (MI)
Stable Angina
Acute Coronary Syndromes (ACS)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 8, 2013; updated Mar 30, 2024 on www.thecalgaryguide.com")
Circle of Willis Anatomy and Physiology

Anterior Cerebral Artery (ACA)
Ischemic stroke (brain damage due to ischemia)
Inadequate blood flow & oxygenation of brain tissue
Occlusion or narrowing
Supplies midbrain, thalamus, & occipital lobe
Posterior Cerebral Artery (PCA) Vertebral Arteries (VA)
Inadequate blood flow & oxygenation of brain tissue
Occlusion or narrowing
Supplies lateral portions of frontal, temporal & parietal lobes (upper extremity & facial regions of motor/sensory cortices)
Middle Cerebral Artery (MCA) P2 segment
A1 segment
Supplies the MCA & ACA
A2 segment
Collateral circulation redistributes blood flow to maintain continuous blood supply
Occlusion or narrowing of vessels within the Circle of Willis
Anterior Communicating Artery (Acomm)
Weakness in the blood vessel walls
Aneurysm formation causes mass effect (displacement) on nearby structures
Supplies BA & PCA, lateral medulla & cerebellum via posterior inferior cerebellar artery (PICA), & upper spinal cord via anterior spinal artery (ASA)
Basilar Artery (BA)
Supplies occipital lobe, cerebellum & brainstem
Thromboembolism (blood clot obstruction)
Inadequate blood flow & oxygenation of brain tissue
Ischemic stroke
Damage to the ventral pons
Locked-in syndrome (quadriplegia, loss of voluntary breathing & speaking, intact cognition & blinking)
Internal Carotid Arteries (ICA)
Posterior Communicating Artery (Pcomm)
Weakness in the blood vessel walls
Aneurysm formation causes mass effect (displacement) on nearby structures
Oculomotor nerve (cranial nerve III): double vision & absent pupil response to light
Legend:
Pathophysiology
Mechanism Sign/Symptom/Lab Finding Complications Published Nov 5, 2018, updated Apr 29, 2024 on www.thecalgaryguide.com
P1 segment
Ruptured aneurysm: subarachnoid hemorrhage
Inadequate blood flow & oxygenation of brain tissue
Hemorrhagic stroke (brain damage due to bleeding)
Optic nerve (cranial nerve II): ↓ visual acuity
Frontal lobe: headache & psychological changes
Authors: Josh Kariath, Rafael Sanguinetti Reviewers: Andrea Kuczynski, Luiza Radu Gary Klein* * MD at time of publication")
Acute Otitis Media Pathogenesis and Clinical Findings in Children

Exposure to tobacco smoke
Impaired macrophage function in nasopharynx
Lack of immunizations
Lack of breastfeeding
Infant does not receive antibodies from breast milk
Overcrowding
Age 6 – 16 months
Immune system deficiencies
Close proximity of kids & ↓ sanitation (e.g. daycare)
↑ Infection risk Upper Respiratory Tract Infection (i.e. bacterial (Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis), viral)
Immature Eustachian tube anatomy which facilitates pathogen transmission to middle ear
Author: Jody Platt Stephanie de Waal Reviewers: Yan Yu Elizabeth De Klerk William Kim Annie Pham Michelle J. Chen Danielle Nelson* * MD at time of publication
Abnormal anatomical structure (e.g. cleft palate)
↑ Nasopharyngeal streptococcus pneumoniae
Lack of immunity to pathogens
↑ Colonization of nasopharynx with bacterial pathogens
Inflammation & edema of respiratory mucosa including the nose, nasopharynx, and Eustachian tube
Obstruction of the Eustachian tube
Air from middle ear resorbs into circulation which creates a low-pressure environment
Negative pressure gradient pulls viral/bacterial pathogens into middle ear
Degenerating white blood cells, tissue debris, and microorganisms accumulate & develops into purulent effusion
Inflammation & infection of middle ear
Complications of acute otitis media**
↑ Pressure in middle ear
Stretching of tympanic membrane
Helper T cells & macrophages release cytokines into the bloodstream
Cytokines trigger hypothalamus to ↑ thermoregulatory set-point
Effusion behind tympanic membrane
Effusion obstructs visualization of ossicles
Neutrophils infiltrate middle ear & phagocytose pathogens
Pus accumulates behind the tympanic membrane
Blood vessels of the tympanic membrane vasodilate
Bulging tympanic membrane
Otalgia (ear pain)
Discomfort disrupts daily activities in young children
Fever
Irritable Poor feeding
Tympanic membrane erythema
Painful blisters on tympanic membrane (e.g. Bullous myringitis)
Can persist for up to 3 months after infection resolves
Loss of tympanic membrane landmarks (i.e. handle of malleus, light reflex)
** See corresponding Calgary Guide slide
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 28, 2013; updated Aug 25, 2024 on www.thecalgaryguide.com")
Cystocele

Connective tissue disorders (e.g. Marfans, Ehlers- Danlos Syndrome)
Genetic susceptibility (e.g. Type III collagen gene abnormality
Menopause
Visceral fat places pressure on pelvic floor structures
Growing fetus places pressure on pelvic floor structures
Straining and bearing down on pelvic floor
Muscle tearing and damage
Disruption of nerves, loss of bladder structural support, and disruption of fascia and muscles
Collagen impairment
Depletion of ovarian follicles leading to ↓ in estrogen production
↑ Intra-abdominal pressure
Transfer of intra- abdominal pressure to pelvic floor
Pelvic floor muscles and pelvic floor fascia become weakened
Pelvic tissue and muscular atrophy
Loss of tissue function and structure support that collagen provided
↓ Stimulation of collagen production
↓ Estrogen levels
Pelvic Organ Prolapse Quantification (POP-Q) System: Grade 1: Bladder descends 1 cm above the hymen Grade 2: Bladder descends to ≤ 1 cm above or below hymen
Grade 3: Bladder descends past the hymen but 2 cm less than total vaginal length
Grade 4: Complete vaginal prolapse
Mechanical obstruction of bladder and urethra
Urinary retention
Descended bladder creates pressure in vagina
Pressure/bulging sensation
Symptoms of voiding dysfunction (e.g. incomplete emptying/frequency/ urgency/nocturia)
Vaginal intercourse puts pressure on descended bladder
Activates pain receptors
Dyspareunia (painful sex) for some patients
Cystocele
Descent of bladder through anterior vaginal wall
Hydronephrosis/ hydroureter
Recurrent UTI
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 5, 2024 on www.thecalgaryguide.com")
Acute Diverticulitis

Obstipation (inability to pass any feces)
Inherent weakness in the muscle layers of the colonic wall associated with immature collagen fibers and diminished wall elasticity
Mucosal and submucosal layers of the colon wall push through a weak spot of the circular muscle layer
Formation of diverticulum (sac-like protrusion of the colonic wall)
Continued stress on diverticula causes micro- perforations of the diverticulum
Inflammation of diverticula
Mesentery and pericolic fat (fat surrounding the colon) attempt to wall off inflammation or perforations
Stool bacteria escapes the colon
Formation of abscess (accumulation of pus in response to the bacteria )
Pro-inflammatory cytokine release from nearby adipose tissue
Hypothalamic thermoregulatory center increases core temperature set point
Fever
Irritation of parietal peritoneum
Inflamed vessels are more permeable and fluid leaks from colonic vessels into the abdominal cavity
Chronic low-grade inflammation triggers activation of pro-fibrotic factors and fibroblasts
Excess production of extracellular matrix proteins
Stimulation of somatic nerves sends pain signals to the brain
Lower left quadrant abdominal pain
Peritoneal signs (abdominal guarding, rigidity, rebound tenderness)
↓ Total circulating blood volume
↑ heart rate
↓ Jugular venous pressure
Orthostatic hypotension (low blood pressure when standing after sitting/lying down)
Gastrointestinal strictures and/or colonic obstruction
Accumulation of micro- perforations further weakens intestinal wall
Complete bowel perforation (medical emergency)
Development of an abnormal connection (fistula) through the bladder, vagina, skin, or gut
Abscesses
Accumulation of fibrotic tissue narrows the intestinal lumen
Fibrosis of colon
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published Oct 4, 2024 on thecalgaryguide.com")
Benzodiazepine mechanism of action

Authors: Tracey Rice Usama Malik Amy Fowler Victoria Silva Reviewers: Sara Cho Keira Britto Luiza Radu Brienne McLane* Aaron Mackie* * MD at time of publication
Benzodiazepine binds to gamma-aminobutyric acid (GABAA) receptors in vascular smooth muscle & the central nervous system (CNS)
↑ Opening of chloride channels
Influx of chloride ions into the neuron Hyperpolarization of nerve membrane causing it to be more negative The cell membrane falls below the normal resting potential
Medulla oblongata inhibition
↓ Respiratory drive; ↓ depth & rate of respirations
Temporary cessation of breathing leads to reduced oxygen supply to the brain
↓ Level of consciousness
Pharyngeal muscle relaxation leading to obstruction
Hypoventilation and/or apnea
General CNS inhibition
↓ Neuronal activity
↓ Electrical brain activity
↓ Seizure activity & hypnotic effect
Thalamic & hypothalamic inhibition
Disruption of short & long- term memory consolidation
Limbic system inhibition
↓ Fear emotions (panic & phobia)
Anxiolytic effect (↓ Anxiety)
Smooth muscle inhibition
Smooth muscles become relaxed &/or less spastic
Vasodilation
↓ Preload Hypotension
↓ Cerebral blood flow
Pre-syncope or syncope
Anterograde amnesia
↓ Visuospatial ability, speed of processing & verbal learning
Confusion
↓ Deep stage of non-REM sleep & delayed REM sleep
Rapid sleep
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 21, 2024 on www.thecalgaryguide.com")
Rapid sequence induction and intubation
: Indications & considerations
“Full stomach”: ↑ risk of regurgitation, vomiting, aspiration Life-threatening injury or illness requiring immediate or rapid airway control
↓ Gastro- esophageal sphincter competence (elderly, pregnancy, hiatus hernia, obesity)
↑ Intragastric pressure (pregnancy, obesity, bowel obstruction, large abdominal tumors)
Delayed gastric emptying (narcotics, anticholinergics, pregnancy, renal failure, diabetes)
↓ Level of consciousness (drug/alcohol overdose, head injury, trauma or shock state)
Respiratory & ventilatory compromise (i.e., hypoxic or hypercapnic respiratory failure)
Achalasia (esophageal motility disorder resulting in impaired swallowing)
Dynamically deteriorating clinical situation (i.e., trauma)
GI bleed
Impaired airway reflexes
↓ Muscle tone of structures in the airway (i.e., tongue, pharyngeal walls, & soft palate)
Patients who did not stop GLP-1 agonist preoperatively as advised
Impaired clearance of secretions or vomitus
↓ Safe apnea time before hemodynamic decompensation
Unprotected airway
Need for rapidly securing airway while avoiding aspiration & hemodynamic compromise
Rapid sequence intubation (RSI): Simultaneous administration of induction agent (unconsciousness) & neuromuscular blocking agent (paralysis) to achieve intubation conditions (~45-60 seconds after IV push) for rapid control of an emergency airway
Preoxygenation
Deranged physiologic conditions (i.e., hypotension, acidosis, hypoxemia)
Reduced tolerance for
apnea (period with no ventilation or oxygenation)
Pre-oxygenate with high flow O2 (15L) to create a large pulmonary & tissue reservoir of oxygen
↓ Significant oxygen desaturation during apnea
↑ Oxygen saturation on pulse oximetry
Induction
Laryngoscopy & intubation are a potent sympathetic nervous system stimulus
Airway manipulation causes a surge in catecholamines
Paralysis
Visualization & passage of endotracheal tube requires relaxation of vocal cords & surrounding muscles
Neuromuscular blocking agents facilitate paralysis
Rescue
Some induction agents (i.e., propofol) are vasodilators
Hemodynamically unstable or patients in shock
Hypotension
Tachycardia
↑ Intracranial pressure (ICP)
Hypertension
Suppress cough & gag reflex
Prevent laryngospasm (involuntary closure of vocal cords to airway manipulation)
Minimize movement during procedure
Vasoactive agents (i.e., ephedrine, phenylephrine) ↑ systemic vascular resistance
Atropine & glycopyrrolate ↑ heart rate
Lidocaine (Na+ channel blocker) & opioids (μ receptor agonist) ↓ transmission of pain
↓ Sympathetic response, myocardial demand & physiologic stress
Anesthetics (i.e., propofol) achieve unconsciousness for paralysis & intubation
↓ Airway trauma & damage to vocal cords
Bag mask ventilation typically avoided in this step to ↓ gastric insufflation & risk of aspiration
Cricoid pressure (Sellick maneuver): posterior displacement of cricoid ring to compress esophagus against C-spine to prevent passive regurgitation of gastric contents to airway. Applied from start of induction, released when placement of endotracheal tube is confirmed by capnography.
Intubation
↑ Blood pressure and/or cardiac output
Authors: Jen Guo Reviewers: Priyanka Grewa Luiza Radu Leyla Baghirzada* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 18, 2024 on www.thecalgaryguide.com")
Acquired Inguinal Hernias

Collagen deficiency
↑ Protease activity Smoking Aging
Malnutrition Collagen breakdown
Long-term glucocorticoid use
Fibroblast (cells which produce collagen) suppression causing ↓ collagen production
Thinning of skin & soft tissues
Incomplete obliteration of the processus vaginalis (peritoneal tunnel through which the testes migrate toward the scrotum during embryological development)
Failed closure leaves an opening for organs to herniate through
Intestinal loops entrapped within herniation
Weakening of connective tissues
Indirect Inguinal Hernia
Protrusion of abdominal and/or pelvic contents through deep inguinal ring
Protrusion of abdominal and/or pelvic contents through the Hesselbach triangle (anatomic area defined by the rectus abdominis medially, inferior epigastric vessels laterally, and the inguinal ligament inferiorly)
Herniated contents become entrapped
Inguinal mass +/- pain that is worse with straining
Abdominal distension & tenderness
Rhythmic contractions of the intestine attempting to push contents past the blockage site
Colicky pain
Incarceration (Surgical Emergency)
Reduced vascular supply to entrapped contents
Strangulation (Surgical Emergency)
Constriction & ischemia of hernial contents
Gangrenous skin changes (swelling, blue/purple colour, ↑ temperature, ulceration, ↓ sensation)
Inflammation of the herniated contents to larger than the hernial opening
Irreducible hernia (a hernia which cannot be manually reduced)
Bowel Obstruction (Surgical Emergency)
Obstruction of intestinal lumen impairs passage of intestinal contents
Stimulation of stretch receptors in the bowel wall
Nausea +/- vomiting
Herniated tissue undergoes necrosis (irreversible cell death), perforating the gastrointestinal wall
Obstipation (complete inability to pass stool or gas)
Bowel perforation (surgical emergency)
Leakage of gastrointestinal contents allows bacteria to infect the abdominal cavity
Sudden ↑ pain
Abscess (localized collection of pus)
Peritonitis (inflammation of the peritoneum)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jun 3, 2018; updated dec 29, 2024 on www.thecalgaryguide.com")
Ptosis

Gravitational effect from excess eyelid weight
Traumatic causes of low eyelid position
Direct injury limits function of LPS or conduction of generated force to the tarsal plate
Laceration of the LPS limiting its function or transection of the levator aponeurosis
Congenital causes of eyelid drooping
Fibrofatty replacement of the LPS muscle at birth
Reduced levator function
eyelid position
Insult to the oculomotor nerve (CNIII) (e.g., compressive, microvascular, demyelinating)
CNIII innervates levator palpebrae superioris, the main muscle responsible for upper eyelid elevation
Insult to the sympathetic innervation (e.g., Horner’s syndrome)
Ocular sympathetic innervate the Muller muscle, which provides approximately 2mm of the upper eyelid’s height
Neuromuscular or myogenic causes of low eyelid position (e.g., myasthenia gravis)
LPS muscle myopathy or defect at its neuromuscular junction that limits the elevation of the eyelid
Aponeurotic causes of low eyelid position
Involutional change (disinsertion) of the levator aponeurosis which connects the LPS to the tarsal plate
Ptosis (also called blepharoptosis)
Abnormally low position of the upper eyelid
↓ distance between the central corneal light reflex (as produced by an examiner’s penlight) and the level of the center of the upper-eyelid margin
↓ Margin-Reflex Distance (Normal: 4-6mm)
Obstruction of the pupil/visual axis
Decreased or occluded superior visual field
↓ distance between the upper eyelid margin and the lower eyelid margin
↓ Palpebral Fissure Height (Normal: 10-12mm)
Flattening of the peripheral cornea by eyelid pressure
Induced with-the-rule astigmatism
Authors: Mina Mina Reviewers: Aicha Djaoutkhanova Shahab Marzoughi Lucy Yang Mao Ding William Trask* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 29, 2024 on www.thecalgaryguide.com")
Pulsus Paradoxus

Thoracic cavity expands
Lungs expand and intrathoracic pressure ↓
Physiologic:
↑ Venous return to right (R) heart
↑ R heart preload (volume of blood inside the ventricle right before it contracts)
↑ Blood pools in the right side of the heart
Obstructive lung diseases (e.g., COPD**, asthma**)
Hyperinflated lungs
↑ Stretching of pulmonary vessels at rest
On inspiration, ↑↑ stretching of pulmonary vessels
↑↑ Blood pools within pulmonary vasculature
↓↓ Flow to L heart
Pathologic: Constrictive pathologies (e.g., cardiac
tamponade**, constrictive pericarditis**) Decreased pericardial compliance
Constriction of ventricles
On inspiration, ↑ venous return to R heart (normal)
R ventricle unable to fully expand due to ↓ compliance
Septum bows into L ventricle
L ventricle unable to fully expand ↓↓ Filling of L heart
↓↓ L ventricular end diastolic volume
↓↓ L heart stroke volume ↓↓ Cardiac output Pulsus Paradoxus
Exaggerated ↓in systolic BP on inspiration (>10mmHg)
Air flows into the lungs
Pulmonary vessels are physically stretched/pulled
↑ Blood pools in pulmonary vessels
↓ Return of blood to left (L) heart
↓ L heart preload
↓ L heart stroke volume
↓ Cardiac output
Obstruction of superior or inferior vena cava (e.g., clot)
↓↓ Venous return to R heart at rest
↓↓ Right heart filling
↓↓ Blood flow to pulmonary arteries
Pulmonary embolism**
Clot occludes pulmonary arteries/ arterioles
↓↓ Flow to pulmonary veins
At rest, ↓↓ flow to L heart
On inspiration, ↓↓↓ flow to L heart
↓ Systolic blood pressure (BP) of < 10mmHg on inspiration
BP = cardiac output x systemic vascular resistance
**See corresponding Calgary Guide slides
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 21, 2013; updated Dec 3, 2024 on www.thecalgaryguide.com")
Constipation in Children

Older Child (>1 years old)
Dietary (e.g., lack of fluids / fiber)
Mechanical (e.g.,. intestinal Atresia, anal atresia)
Congenital malformation (narrowing, absence, or malrotation) of structure of intestine / anus
Interrupted flow of bowel contents
Genetic (e.g., cystic Fibrosis)
Mucous blocks pancreatic duct
Inability of pancreatic enzymes to reach small intestine
↓ Digestion after a meal
Large, thickened stool
Neurologic (e.g., Hirschsprung's disease)
Congenital disruption of the migration of neural crest cells to the distal colon
Affected segment of the colon fails to relax
Progressive secondary dilation of the healthy proximal colon
Systemic (e.g., hypothyroidism)
Thyroid hormone deficiency
Reduction in the stimulation of gut tone & contractility by thyroid hormones
↓ Peristalsis (intestinal contractions) of the bowel
Dietary
(e.g., lack of fluids/ fiber)
Mucosal (e.g., celiac disease)
Inappropriate immune response against gluten
Intestinal mucosal injury
Malabsorpti on of water and other nutrients
Functional (e.g., pain)
Prolonged stool retention in bowel
↑ Time in bowel causing over- absorption of water from stool into the large intestine
Mechanical (e.g., bowel obstruction)
Mechanical obstruction in the intestines
Interrupted flow of bowel contents
Intestinal obstruction
Neurologic (e.g., neglect, physical abuse)
Disturbance in brain-intestine axis
Mechanisms not fully understood
Visceral hyper- sensitivity
(increased pain sensation)
Withholding behaviour
Lack of soluble fiber
↓ Attractive forces between water & stool
Prevention of secretion of water into stool
Lack of insoluble fiber
↓ Stool bulk and laxation
↓ Secretion of water &
mucous into stool
Lack of soluble fiber
↓ Attractive forces between water & stool
Prevention of secretion of water into stool
Lack of insoluble fiber
↓ Stool bulk and laxation
↓ Secretion of water & mucous into stool
Formation of dry & hard stool
Formation of dry & hard stool
Difficulty passing stool
Difficulty passing stool
Authors: Jennifer Wytsma Reviewers: Sophia Khan, Shahab Marzoughi, Sylvain Coderre* * MD at time of publication
Intestinal obstruction
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Dec 15, 2024 on www.thecalgaryguide.com")
Pituitary Tumour Classification and Clinical Outcomes
 (lack of hormone-producing cells or due to gene mutations)
Authors: Chris Oleynick Caroline Kokorudz Reviewers: Amyna Fidai Laura Byford- Richardson Joseph Tropiano Julia Gospodinov Luiza Radu Hanan Bassyouni* * MD at time of publication
hormones (70%)
Relative abundance & predisposition for lactotroph (prolactin-producing), somatotroph (growth hormone – producing), thyrotroph (TSH producing) & corticotroph (adrenocorticotropic hormone – producing) cells to form adenomas (epithelial cell tumours)
↑ Lactotroph cells
↑ Prolactin (PRL) (most common)
Hyper- prolactinemia (high prolactin blood levels)
↑ Somatotroph cells
↑ Growth hormone (GH)
Acromegaly* (excess tissue growth & metabolic dysfunction)
↑ Corticotroph cells
↑ Adrenocortico- tropic hormone (ACTH)
Cushing disease* (prolonged exposure to excess cortisol)
↑ Thyrotroph cells
↑ Thyroid stimulating hormone (TSH)
Central hyper- thyroidism (↑ T4 & T3)
Large size (macro) (>10mm on MRI) may cause mass effect (tissue compression from mass)
Small size (micro) (<10mm on MRI) unlikely to cause mass effect (compression to surrounding structures)
Asymptomatic
Headache
Nausea & vomiting
Compresses pituitary gland & impairs blood supply & function of pituitary cells
Impinges pituitary stalk & disrupts hormone transport from hypothalamus to the anterior and posterior pituitary
Compresses surrounding structures
↑ Pressure & stretching of dural mater
Stretching of the meninges activates mechanoreceptors (stretch receptors) in GI tract
Pituitary hormone deficiency (typically in left-right order with mass effect):
Dopamine release obstruction
↓ Inhibition of prolactin secretion
Antidiuretic hormone (ADH) obstruction
Inferior tumour growth
Growth into sphenoid sinus
Lateral growth of the tumor compresses surrounding cranial nerves
Superior tumour growth
↓ GH
↓ Protein production & muscle cell proliferation
↓ Luteinizing hormone (LH) (triggers ovulation & sex hormone synthesis) & follicle stimulating hormone (FSH) (stimulates ovarian follicles & sperm growth)
↓ (TSH)
↓ ACTH (stimulates cortisol & androgen release)
Cranial nerve (CN) II (optic)
↓ Visual acuity
Diplopia (double vision)
CN III, (oculomotor) IV (trochlear), or VI (abducens)
Ptosis* (drooping upper eyelid)
CN V (trigeminal) branches V1 & V2
Facial numbness
Ophthalmoplegia (eye muscle paralysis)
Compresses optic chiasma
Bitemporal hemianopsia (decreased lateral peripheral vision)
Tumour extends into hypothalamus
Hypothalamic dysfunction due to damage to hypothalamic cells
Disruption of multiple regulatory systems (i.e. sleep-wake cycles, appetite, temperature)
Tumour occludes ventricles
Tumour obstructs CSF flow
↑ Intracranial pressure
Hydrocephalus* (abnormal buildup of CSF in ventricles of the brain) and papilledema
Bacteria migrates from sinus flora into sphenoid sinus
Cerebrospinal fluid (CSF) leaks into throat
Post-nasal drip and nasopharyngeal mass
Stunted growth and short stature in children
↓ Muscle mass & fatigue
Diabetes insipidus* (excessive urination & extreme thirst)
Central hypothyroidism* (↓ T4 & T3)
Hyperprolactinemia
Meningitis* (inflammation of the meningeal layers of central nervous system)
*See relevant Calgary Guide slide
Hypogonadotropic hypogonadism (↓ Sex hormones)
Adrenal insufficiency* (↓ 8 AM cortisol)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 1, 2027; updated Jan 5, 2025 on www.thecalgaryguide.com")
Acute Infectious Mononucleosis
, Cytomegalovirus
(CMV), human immunodeficiency
virus (HIV), etc) through saliva
(most commonly in adolescents
& young adults aged 15-24)
Virus infects epithelial
cells of the oropharynx
Virus infects & immortalizes
circulating B lymphocytes
Virus replicates in infected B-cells
Immune cell proliferation
in lymphatic system
(primarily lymph nodes & spleen)
Infected B-cells enter
systemic circulation
Systemic inflammatory
response activated
Inflammation &
edema of sinuses
Bilateral periorbital &/or palpebral edema
Pharyngitis**
(often with grey/white
exudative secretions)
Palatal petechiae
Blood vessel damage
in the soft palate
Edema of soft palate & tonsils
Airway obstruction
↑ Immunoglobulin M (IgM) antibodies
to EBV viral capsid antigen (VCA) Positive IgM-VCA
Immortalized B-cells
produce ↑ antibodies
Production of heterophile antibodies
(weakly reactive & non-specific)
Positive monospot (heterophile antibody)
test (↓ sensitivity in children <4 years)
Virus may remain dormant in B-cells
Latent infection with periodic reactivation
Generalized lymphadenopathy (enlarged lymph nodes)
Massive cervical, mediastinal or hilar lymphadenopathy
Posterior cervical
lymphadenopathy
Platelets sequestered (trapped) within spleen &
overactive spleen (hypersplenism) discards ↑ platelets
Thrombocytopenia
(↓ platelets)
Weak reticular tissue in the spleen stretches
Splenomegaly Splenic rupture
& becomes more susceptible to injury
Inflammatory response ↑ energy demand
Fatigue
Longstanding impacts from
unknown mechanism Chronic Fatigue Syndrome
Inflammatory cytokines
released into circulation
↑ Thermo-regulatory
set-point at hypothalamus Fever
Lymphocytosis (↑ lymphocytes)
(markedly CD8+ T-cells & NK cells) Immune cells infiltrate the liver Hepatomegaly
↑ Aminotransferases
Leukocytosis (↑ leukocytes)
CD8+ T-cells & NK cells
indirectly damage hepatocytes
↑ Bilirubin & jaundice**
Systemic immune response &/or
antibiotic hypersensitivity reaction
CD8+ T-cells
respond to virus
Atypical lymphocytes
on blood smear
Generalized maculopapular rash
Authors:
Ayden Hansen, Griselle Leon
Reviewers:
Charissa Chen, Emily J. Doucette
Danielle Nelson*
* MD at time of publication
Published Sept 3, 2015; updated Apr 22, 2025 on www.thecalgaryguide.com
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications")
Tetralogy of Fallot

Maternal exposure
to alcohol or
anticonvulsants
Maternal infections (e.g., hepatitis
B virus, coxsackievirus-B, human
cytomegalovirus virus, rubella)
Variable interaction between genetic associations and environmental risk factors
Antero-cephalad deviation of conal septum (muscular structure that forms the boundary
between right & left ventricular outflow tract during embryological development)
Tetralogy of Fallot
Cyanotic congenital heart disease with a combination of four cardiac defects
Ventricular septal
defect (VSD)**
Overriding aortic root
(aorta above VSD rather than left ventricle)
Right ventricular outflow
tract obstruction (RVOTO)
Right Ventricular
Hypertrophy
Hole in septum
Absent or reduced
Stressors (eg., crying,
between ventricles Right ventricle of
Oxygenated blood from the left
pulmonary valve
defecation, fever,
heart pumps
ventricle and deoxygenated blood
closure (P2)
dehydration) trigger acute
harder to push
from right ventricle flows into aorta
↑ Left ventricular
pressure
infundibular spasm (spasm of
blood through
conus arteriosus)
RVOTO
Chronic volume
overload
L-R ventricular
shunting
Single, loud S2
Spasm ↓ blood flow through
right ventricular outflow tract
Aortic
Dilated
aortic root
regurgitation** Hypercyanois or “tet” spells
Turbulent blood
flow from left
ventricle through
the hole in septum
to right ventricle
Turbulent diastolic
backflow through
incompetent aortic
valve
Deoxygenated
blood flows
through aorta to
systemic circulation
↓ O2 Saturation
Chemoreceptors in the carotid & aortic bodies
stimulate respiratory centre in the medulla oblongata
Harsh, holosystolic
murmur
Diastolic
decrescendo
murmur
↑ Deoxygenated blood
entering systemic circulation
↑ Catecholamine release from adrenal
medulla stimulating ↑ contractility of heart
↓ Blood flow
across VSD
↑ contraction against outflow obstruction
↑ pulmonary vascular resistance
↓ Intensity or
disappearance
of holosystolic
murmur
Peripheral & central
chemoreceptors detect ↓ arterial
O2 content, triggering brainstem
respiratory centre to stimulate ↑
work & rate of breathing
↓ Pulmonary blood flow
↑ Turbulence of blood
flow through RVOTO
↑ R-L shunting
↑ Deoxygenated hemoglobin (dark
red) relative to oxygenated hemoglobin
(bright red), reflecting more blue light
Cyanosis (blue discoloration of the
mucous membranes, nail beds, skin)
Paroxysmal
hyperpnea (rapid
and deep
respirations)
Irritability
and crying
Dyspnea
(shortness of
breath)
Poor feeding
Accentuation of systolic
crescendo/decrescendo
murmur with harsh ejection
**See corresponding
Calgary Guide slides
Legend: Mechanism
Published Jul 8, 2015; updated Jun 16, 2025 on www.thecalgaryguide.com
Pathophysiology Sign/Symptom/Lab Finding Complications")
Unconjugated Hyperbilirubinemia
 factor
incompatibility
Maternal sensitization
against Rh-positive fetal cells
Maternal antibodies against Rh
factor attack fetal RBCs
ABO incompatibility
Native maternal antibodies against non-
native blood types attack fetal RBCs
Sepsis** Widespread systemic inflammation Cytokines & complement factors damage RBC membranes
Disseminated intravascular
coagulation** (clotting
proteins become overactive)
Clots form in
systemic circulation
Small clots shear & damage
RBCs in circulation
Red blood cell
(RBC) enzyme
defects
Glucose-6 phosphatase
dehydrogenase (G6PD)
deficiency**
G6PD protects RBCs against
oxidative damage
↑ RBC sensitivity to oxidative
stress (during acute stressors)
Pyruvate kinase
deficiency (PKD)
Abnormal glycolysis & cellular
energy production
↓ RBCs life spans
RBC membrane
defects
Hereditary spherocytosis
RBCs are abnormally round (spherocytes)
RBC
membranes
easily damaged
in circulation
Bilverdin reductase
Hereditary elliptocytosis
RBCs are abnormally elongated or oval
converts bilverdin to
Sickle cell
Abnormal hemoglobin (HbS)
RBCs become abnormally
unconjugated bilirubin
disease**
polymerizes under ↓ O2
sickle shaped
Hemoglobinopathies
Thalassemia's**
Defective hemoglobin
chains in RBCs
Irregularly
shaped RBCs
trapped in
spleen
RBC
sequestration
↑ Production of RBCs (Polycythemia**)
Accumulation of blood (i.e.
Cephalohematoma, hemorrhage)
↑ RBC load &
turnover
Causes of ↓
hepatocellular
bilirubin clearance
Genetic defects in
uridine diphosphate
glucuronosyltransfe
rase (UGT) enzyme
(conjugates
bilirubin in liver)
Gilbert syndrome
Unconjugated bilirubin
↓ UGT production
remains insoluble & cannot
Crigler–Najjar
be excreted in bile
syndrome Type II
Crigler–Najjar
syndrome Type I
No UGT production
Breast milk jaundice Breast milk contains β-glucuronidase
Causes of ↑
entero-hepatic
bilirubin circulation
Intestinal obstruction
Obstruction blocks bile flow from liver to intestines Breastfeeding
jaundice
Inadequate milk intake (volume
depletion/dehydration)
↑ Reabsorption of bilirubin
in the intestines
**See corresponding Calgary Guide slide
Legend: Macrophages engulf
old or damaged RBCs
in spleen & liver
↑ Hemolysis (RBC
breakdown)
RBCs release cellular
contents including heme
(from hemoglobin)
Heme oxygenase
converts heme to
bilverdin
↑ Unconjugated
(indirect) bilirubin
accumulation in blood
↑ Total serum
bilirubin levels
Excess bilirubin
deposition into elastin-
rich tissues (eg. skin,
sclera) due to ↑
affinity for elastin
Pathologic neonatal jaundice
(yellow discoloration of skin
within first 24 hours of life)
Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications
Published July 13, 2025 on www.thecalgaryguide.com
Authors:
Merry Faye Graff
Khushi Arora
Reviewers:
Annie Pham
Emily J. Doucette
Danielle Nelson*
* MD at time of publication
Hemolytic
anemia**
↓ Bilirubin
conjugation
β-glucuronidase deconjugates bilirubin
Bilirubin builds up
in hepatic system
Unconjugated
bilirubin crosses
blood-brain barrier
Bilirubin-induced
neurologic
dysfunction (BIND)
Kernicterus (bilirubin-
induced neurological
damage)
Scleral icterus
(yellowing of
sclera in eyes)")