Notice: Undefined variable: out in /web/sites/calgaryguide_current/wp-content/themes/cg-new/functions.php on line 570
SEARCH RESULTS FOR: calcium
Nephrotic Syndrome: Pathogenesis and Clinical Findings
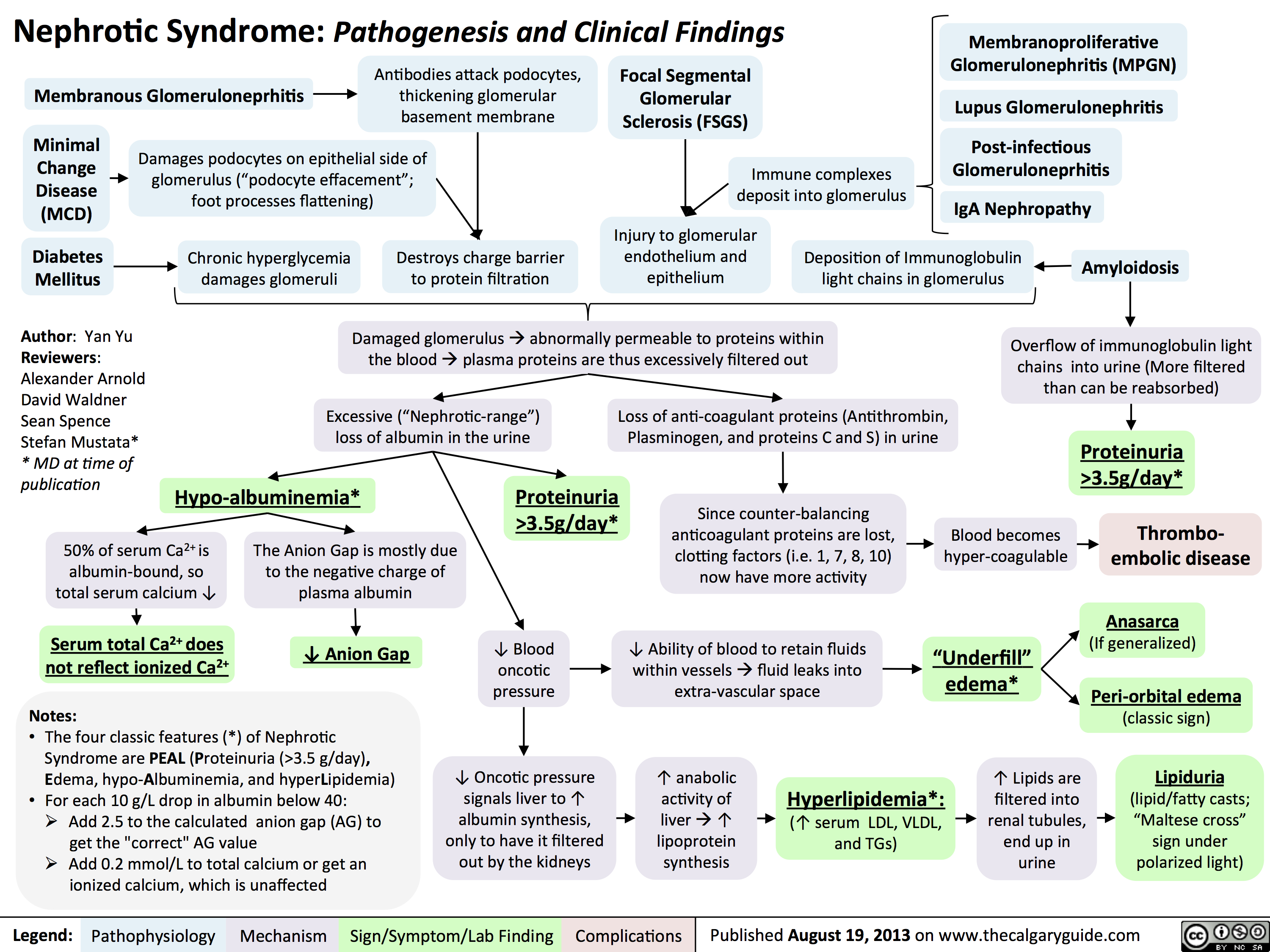 3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
Hypercalcemia - Clinical Findings
![Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hypercalcemia-Clinical-Findings.jpg "Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be")
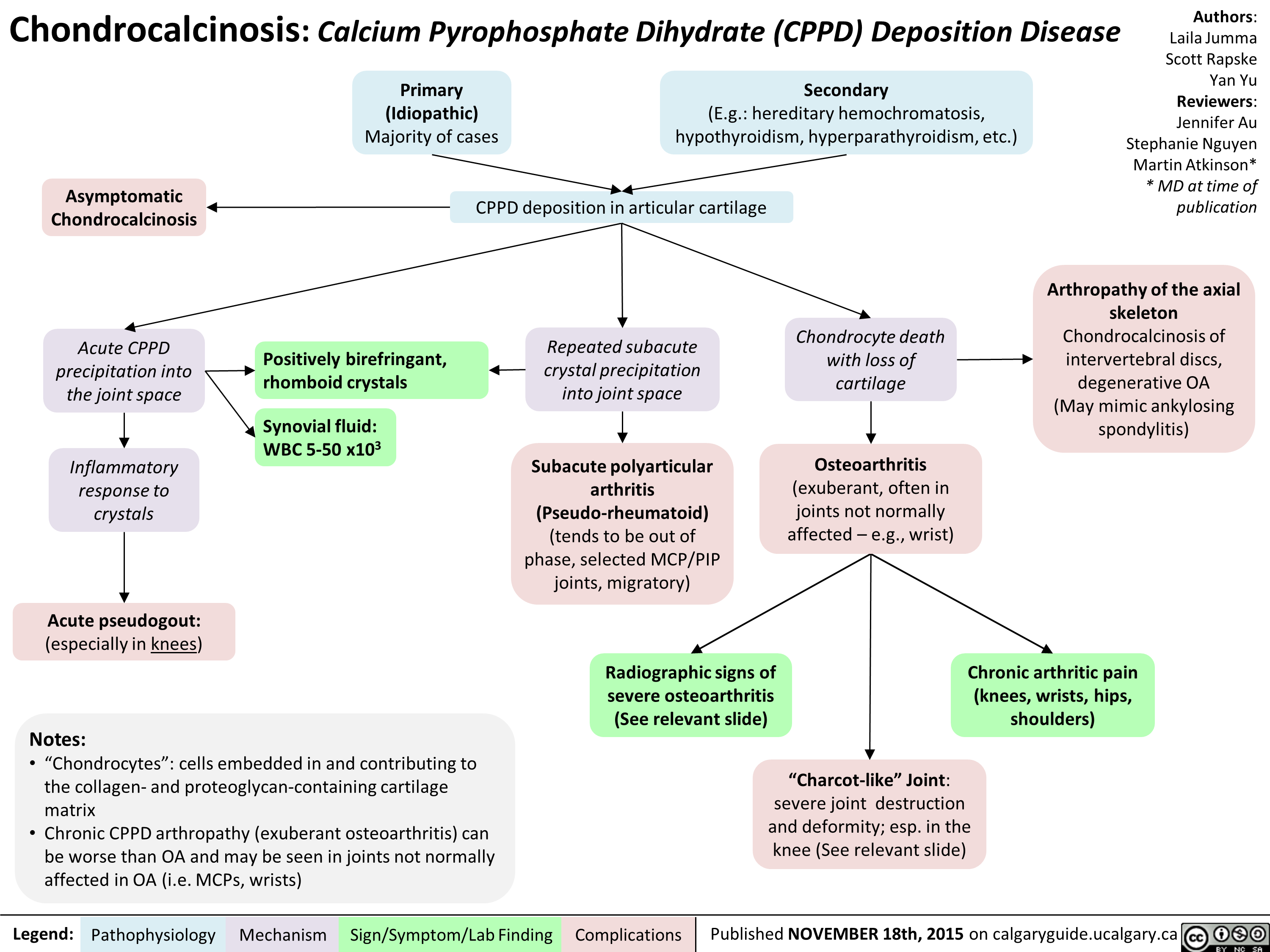
Chondrocalcinosis Calcium Pyrophosphate Dihydrate Deposition Disease
Lung cancer clinical findings and paraneoplastic syndromes

Obstruction of proximal airway
Inability to clear inhaled pathogens Postobstructive pneumonia
Cough, fever, dyspnea
Local tumor growth
Spread of tumor to pleural surface
Chest Pleural discomfort effusion
• Obstruction or compression at local site
Uncontrolled abnormal cell growth in one or both lungs 4 Lung Cancer
Airway invasion
Hemoptysis
Lambert-Eaton syndrome (Production of auto-antibodies against Calcium channels)
Muscle weakness
I` effort to Compression at the Compression Superior vena ventilate the laryngeal nerve of brachial cava lungs nerve plexus compression Impaired innervation to the vocal cords Dyspnea Shortness of Arm/shoulder/ Face/arm breath Voice hoarseness neck pain edema
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Authors: Yoyo Chan Reviewers: Midas (Kening) Kang Usama Malik Leila Barss* * MD at time of publication
Tumor secretes biologically active substances
Paraneoplastic Syndromes 4 Associated symptoms with malignant diseases
TGF131 extracellular matrix protein
Fingers clubbing
PTHrP T calcium release from bones
Hypercalcemia Serum calcium >2.6 mmol/L
ADH 1 SIADH T water reabsorption 1
Hyponatremia Serum sodium <135mEq/L
Abbreviations: • ACTH: Adrenocorticotropic hormone • ADH: Anti-diuretic hormone • PTHrP: Parathyroid hormone-related protein • SIADH: Syndrome of inappropriate antidiuretic hormone production • TGFI31: Transforming growth factor beta 1
1` ACTH
cortisol release and production
Cushing's syndrome (symptoms and signs caused by prolonged cortisol exposure)
Muscle weakness, hyperglycemia, severe hypokalemia")
Celiac Disease: Complications
 Carbohydrate Protein Fat Secretory maldigestion maldigestion malabsorption diarrhea
Legend:
Fermentation by gut bacteria 1 Gas production
Bloating
Fat retained in stool
Steatorrhea
Abdominal pain
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Growth Retardation
Authors: Yoyo Chan Reviewers: Peter Bishay Usama Malik Sylvain Coderre* * MD at time of publication
IgA response
Autoimmune IgA deposits Lymphocyte response in sub-epidermal skin layer against enamel
Dermatitis Herpetiformis (Chronic pruritic blisters)
Nutritional deficiency
Dental enamel hypoplasia
Vitamin D and calcium deficiency
Zinc, selenium Folate Iron Osteoporosis deficiency deficiency deficiency Anemia t Risk of miscarriages")
Neuromuscular Junction (NMJ)- Physiology and pharmacology
- Physiology and pharmacology calcium ion ions voltage gated ca2+ channels acetylcholine ACh receptors nicotinic SNARE protein complex AChR receptor sodium muscle specific kinase action potential voltage gated Ca2+ channels activated release presynaptic terminal binds")
Rickets and Osteomalacia: Pathogenesis and Clinical Findings

Shear forces
bend the
osteopenic
bone
Short stature
Diffuse skeletal pain
(bone tenderness)
Osteopenia
reduces bone
density and
cause fractures
with minimal
force applied
If hypophosphatemic,
production of ATP and
other high energy
molecules declines
Unequally
distributed
forces and
muscle/tendon
tension
stimulate
nociceptors
Legend: Published November 26, 2012 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Calcification inhibitors
(excess exposure to Al,
Fluoride, etidronate)
Lack, or reduced
function, of
mineralization
enzymes (like ALP)
Lack of bone mineral components:
1. Phosphate: renal tubule disorders, vit D
or Phosphate deficiency, ↑FGF23
2. Calcium: severe deficiency (infants)
Rickets: Occurs before
epiphyseal closure
Epiphyseal
plates do not
fuse, impairing
bone growth
Bowed legs
Cartilage in epiphyseal
plates cannot become
ossified
Disruption in
calcium ion
homeostasis
↓ GI
absorption of
Ca2+ into
blood
↓ Kidney
reabsorption
of Ca2+ into
blood
↓ energy available
to muscle
Author:
Payam Pournazari
Reviewers:
Yan Yu
Spencer Montgomery
David Hanley*
* MD at time of
publication")
Crohn's Disease

Inflammation of the GI tract lining
- Inflammation is “transmural”, spanning the entire thickness of the intestinal wall from luminal mucosa to the serosa.
- The inflammation occurs anywhere in the GI tract from the oral mucosa to the anal mucosa (from ‘gums to bum’) in skip lesion pattern.
Atrophy, scarring of the intestinal villi
Inflammatory cytokines destroy the mucosa epithelial cells of the GI tract wall, causing cell apoptosis and ulceration
↑ permeability of the blood vessels supplying the GI tract wall
Chronic inflammation impairs healing responses
Dysregulated wound healingàexcess
extracellular matrix deposition
Fibrosis leads to scar tissue and thickening of all layers of the GI tract
Strictures
Inflammation is systemic, affecting:
Joints Arthropathy Erythema
Impaired absorption of nutrients
Weight loss
Prolonged GI bleeding
Anemia
Transporter proteins responsible for Na+ reabsorption gradually disappear from the epithelium
More sodium (and thus water) is
retained in the GI tract lumen
Microperforations can penetrate through the intestinal wall
Anal fistulae (“holes” connecting the anus to the skin, bladder, peritoneum, small bowel, etc.)
Continued inflammation and/or infection can lead to:
Leakage of fluid out of capillaries into the GI tract
Luminal edema and swelling
Narrowing of GI lumenàbowel obstruction
Skin
Mouth Eyes
Liver
nodosum, pyoderma gangreno- sum
>5 canker sores
Uveitis
Iritis, scleritis
Sclerosing cholangitis
↓ fat absorption
Fatty acids (negatively charged) bind Ca2+, freeing oxalate from Ca2+
↑ oxalate absorbed into blood & filtered by kidney
Calcium oxalate kidney stones
Diarrhea
Abdominal cramping and pain
(see Bowel Obstruction page for full mechanism
Anal abscesses Inflammatory masses
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Multiple-Myeloma
 immunoglobulins
Normal SPEP: no spike in the gamma (γ) region
Notes:
• MGUSismuchmorecommon than MM!
• “Plasmacell”:Blymphocytes that produce antibodies/ immunoglobulins
Stimulation by specific antigens
Genetic changes/mutations accumulate over time in one type of plasma cell
Abbreviations/Definitions: • SPEP - Serum Protein
Electrophoresis
• Ig – Immunoglobulin • Monoclonal – “of one
specific genetic strain or subtype”
One type of plasma cell starts to proliferate abnormally
Monoclonal Gammopathy of Undetermined Significance (MGUS) (Premalignant, mild monoclonal plasma cell proliferation; asymptomatic)
In 1-2% of cases, further cytogenetic changes over time stimulate further proliferation of this plasma cell line
Multiple Myeloma (MM)
(extensive monoclonal B lymphocyte proliferation, causing end organ damage)
Slightly more monoclonal plasma cells will produce slightly more monoclonal Immunoglobulins
Small spike in the gamma (γ) region of the SPEP (less prominent compared to the spike in MM)
More monoclonal plasma cells result in far greater amounts of monoclonal immunoglobulins being secreted
Large spike in gamma (γ) region of the SPEP
Ig light chains accumulate in the tubules of kidney nephrons
Light chain casts obstruct tubules
Renal Insufficiency (↓GFR)
Osteoblasts ↑ expression of RANK-ligand (RANKL, an apoptosis regulator), and ↓ expression of Osteoprotegerin (OPG, a decoy receptor for RANKL)
↑ osteoclast activity vs osteoblast activityàbone loss
Clonal plasma cells overrun normal bone marrow, crowding out production of red blood cells, ↓ red blood cell counts
Anemia
Authors: Tristan Jones, Tyler Anker, Yan Yu Reviewers: Jennifer Au, Crystal Liu, Man- Chiu Poon*, Lynn Savoie* * MD at time of publication
Damaged bones hurt, & become more brittle
Bony pain, pathologic fractures
Osteolytic bone lesions
Osteoclasts release calcium from bone and into blood
Hypercalcemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 12, 2020 on www.thecalgaryguide.com")
Pseudogout
 crystals from joints is inhibited by iron
Hypomagnesia
The relative absence of magnesium impairs pyrophosphatase activity, reduces pyrophosphate breakdown
Hypophosphatasia
Defective mineralization of calcium and phosphorous in bones
Idiopathic (vast majority of cases)
Mechanism unknown
↑ serum concentrations of Ca2+ or Pyrophosphate
Enhanced mineralization in chondrocytes (cells that make cartilage)
Abbreviations
• NTPPPH nucleoside triphosphate
pyrophosphohydrolase
• CPPD – Calcium Pyrophosphate
Dihydrate
Notes:
• There are different types of calcium pyrophosphate crystal deposition (CPPD) disease. This slide only covers “pseudogout”.
• Pyrophosphate (PPi) = 2 phosphate molecules = P2O74−
• Pyrophosphate is made from the breakdown of Adenosine triphosphate (ATP): ATP -> AMP + PPi
Once in cartilage, high levels of either calcium ions or pyrophosphate can result in them binding together, forming CPPD crystals
Aggregated CPPD crystals shed into synovial fluid
Neutrophils enter joint to phagocytose the crystals and release pyrophosphatase enzyme
Repeated crystal precipitation into joint space over time (subacute process)
CPPD crystals collect on collagen fibers in articular cartilage
Chondrocalcinosis, seen on high-resolution ultrasound and/or x-ray
CPPD crystals exhibit unique properties on polarizing microscopy
Inflammatory cascade
Positively birefringent (crystals appear blue parallel to axis of polarizer)
PAINFUL, warm, swollen joint (sudden onset)
↑ C-reactive protein (CRP); erythrocyte sedimentation rate (ESR)
Knees and wrist subjected to more trauma over a person’s lifetime
Knee > Wrist >>> any other joint affected
Wearing down of joint cartilage over time
Rapidly progressive osteoarthritis (see osteoarthritis slide)
Subchondral sclerosis & cysts, joint space narrowing, and osteophytes seen on x-ray
bone loss, hemarthrosis
Nerve damage over time
“Charcot-like” joint: severe weightbearing to areas that joint destruction/deformity,
Painless joint
Lack of sensation can cause tolerate it poorly
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 16, 2020 on www.thecalgaryguide.com")
GI-changes-during-pregnancy
 Tract
Pregnancyàhormonal and physical changes in the body
Mechanisms poorly understood
↑ human chorionic ↑ estrogen ↑ progesterone gonadotropin (hCG)
↑ uterus size
Uterus rises into
abdominal cavity
↑ intra-gastric pressure
↑ backup of stomach contents
Nausea & vomiting
In the extreme case:
Hyperemesis gravidarum (extreme vomiting causing weight loss, dehydration, ketosis)
Liver displaced upwards
Liver edge generally not palpable on exam
↑ blood pressure in veins within the abdomen
Veins around rectum & anus stretch under pressure
↑ blood flow to the gum tissue
↑ tendency for gingival bleeding & ulceration
Gingivitis
↑ neo- vascularization in lesions on skin
Pyogenic granuloma of pregnancy (shiny red papule with a raspberry-like surface)
Mechanism poorly understood
Ptyalism (excessive salivation)
Difficulty swallowing excess saliva
↑ gallbladder stasis
Biliary
sludge given time to solidify within gallbladder
Gallstones
↓ mobilization of intracellular calcium within smooth muscle cells
Smooth muscle relaxation in tissues such as the gallbladder & GI tract
Changes in taste perception
Dysgeusia
Cultural influences and psychological factors
Change in diet and dietary cravings
↓ lower esophageal sphincter tone
Retrograde transport of gastric contents into esophagus
Gastroesophageal reflux
↓ GI motility
Delayed gastric and intestinal emptying
Stool builds up in colon, and hardens as water is resorbed
Constipation
Pooling of blood within rectal veins àvenous thrombosis
Hemorrhoids
Fragile veins, more easily torn
Rectal bleeding
Change in gut microbiome
Authors: Simonne Horwitz, Yan Yu*
Reviewers: Claire Lothian, Crystal Liu, Ronald Cusano* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 29, 2020 on www.thecalgaryguide.com")
Placenta-Previa

• If patient presents with bleeding, a pelvic exam = risk of damaging placentaàmore bleeding
• Use transvaginal ultrasound to confirm location of placenta
Previous C/S Multiple gestation Maternal smoking
Placenta Previa
Presence of placental tissue that extends over the internal cervical os. (Pathogenesis unknown; preceding textboxes are risk factors only)
Previous placenta previa Increased maternal age Increased parity
Total placenta previa
Placenta completely covers the cervix
Partial placenta previa
Placenta covers cervix partially
Marginal placenta previa
Placenta near the edge of the cervix
Diagnosed early in pregnancy on routine abdominal ultrasound at 18-20 weeks Stretching of lower segment of uterus during 3rd trimester
OR
Alternate scenario:
One scenario:
This stretching elongates the space between the cervix and the placenta, relocating the stationary lower edge of the placenta away from the cervical os
Placenta previa resolves on its own
Reassuring: Placenta >2cm from cervical os on ultrasound
This stretching fails to move the placental away from the cervical os
Previa persists as uterus changes in preparation for labour:
Thinning of the lower segment of the uterus
Uterine contractions
Shearing forces to the placental attachment site
Painless bright red vaginal bleeding (90%)
↑ risk of clinically significant hemorrhage
Cervix becomes thinner (effaced) and opens (dilates)
Bleeding limits oxygen delivery to placenta, injuring placental tissue
Tissue injuryàActivates intracellular G-protein signalling pathways
Release of stored intracellular calcium àmyometrial contraction
Uterine contraction and bleeding (10%)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 2, 2020 on www.thecalgaryguide.com")
Anesthetic-Considerations-Aortic-Stenosis
 for Patients with Aortic Stenosis Undergoing Non-Cardiac Surgery
CRRAP Goals:
Contractility, Rate, Rhythm, Afterload, Preload
Pathophysiology Driving Anesthetic Management Hemodynamic Anesthetic Intervention (CRRAP) Goals
Author:
Ryan Brenneis Reviewers: Stephen Chrusch Hannah Yaphe Yan Yu*
Karl Darcus*
* MD at time of publication
Aortic stenosis = Narrow aortic valve opening
Notes:
-Cardiac Output = Heart Rate x Stroke Volume
-Stroke volume has 3 determinates:
1. Contractility 2. Afterload
3. Preload
If the patient’s heart cannot ↑ contractility to maintain cardiac output...
↑ resistance to forward blood flow àheart must ↑ its contractility (↑ the forcefulness of its contractions) to overcome this resistance
Applying ↑ force over time causes left ventricle to undergo concentric hypertrophy
Contractility deteriorates over time
Heart rate must compensate for maintaining cardiac output
Coronary Perfusion Pressure = Diastolic BP (DBP) – Left Ventricular End Diastolic Pressure (LVEDP)
↑ cardiac muscle massà↑ myocardial metabolism and oxygen demand
↑ left ventricular wall stiffnessà↓ LV filling while relaxed (diastolic dysfunction)
Intraoperative ↓ in contractility compromises cardiac output
Bradycardia ↓ cardiac output
Tachycardia ↓ filling time of left ventricle (↓ preload)
Coronary perfusion occurs during diastole
Coronaries require a high DBP to maintain perfusion
Tachycardia ↓ perfusion time
Hypotension ↓ coronary perfusion pressure
Possible myocardial ischemiaà ↓ blood pumped into vessels
40% of LV preload supplied from atrial kick
Loss of atrial kick with arrhythmias à↓ cardiac output
Note: Aortic stenosis severity (see slide on aortic stenosis) and the type/risk of surgery guide the hemodynamic consequences and need for intervention
Adequate intravascular volume required to passively fill stiff ventricle
Contractility
↓ use of negative inotropic Maintain drugs, e.g. calcium channel
contractility blockers (“Inotrope”: drug that alters heart’s contractility)
Rate
Keep heart rate above 60 bpm
Keep heart rate below 80 bpm
Consider transcutaneous pacing, anticholinergics, & sympathetic agonists
↑ anesthetic depth, consider beta blocker (e.g. Esmolol)
Afterload
Maintain a Mean Arterial Pressure >70mmHg
Consider sympathomimetic drugs to treat hypotension
Monitor blood pressure closely via arterial line
Consider increasing anesthetic depth for severe hypertension
Rhythm
Maintain Sinus Rhythm
Consider presurgical placement of defibrillator pads & crash cart
Amiodarone ready & available during operation, to terminate any arrhythmias
Preload
Maintain Euvolemia
Possible use of transesophageal echo to monitor preload
Ensure adequate venous access- consider central venous catheter and large bore IV’s
Legend:
Pathophysiology
Mechanism
Goal
Anesthetic Intervention
Published October 25, 2020 on www.thecalgaryguide.com")
Tumour-Lysis-Syndrome

Though rare, aggressive tumours can spontaneously lyse without treatment
Intracellular potassium released into bloodstream
Intracellular phosphate released
Hyperphosphatemia
↑ serum phosphate
Intracellular lactate dehydrogenase (LDH) released
↑ serum LDH
Intracellular nucleic acids released
Nucleic acids metabolized to uric acid
Hyperuricemia
↑ serum uric acid
Hyperkalemia
↑ serum potassium
(see Hyperkalemia: clinical findings)
Uric acid (a crystallizing substance) ↑ precipitation of calcium phosphate
↑ filtration of poorly soluble uric acid into acidic environment of renal tubules
Serum phosphate binds serum calcium, forming solid calcium phosphate precipitate crystals
High levels of calcium phosphate ↑ uric acid precipitation
Uric acid precipitates as crystals and deposits in kidney tubules and collecting ducts
Tubular injury and/or intraluminal obstruction
Endothelial dysfunction in renal vasculature
Renal inflammation, vasoconstriction, and
impaired renal vascular autoregulation
Decreased renal filtration
Acute Kidney Injury
(see Acute Kidney Injury Overview)
Crystal deposition in the heart
Depletion of soluble calcium
Hypocalcemia
Calcium phosphate crystals deposit in kidneys
Main mechanism of Acute Kidney Injury
Cardiac Arrythmias
↓ serum calcium
(see Hypocalcemia: clinical findings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 25, 2020 on www.thecalgaryguide.com")
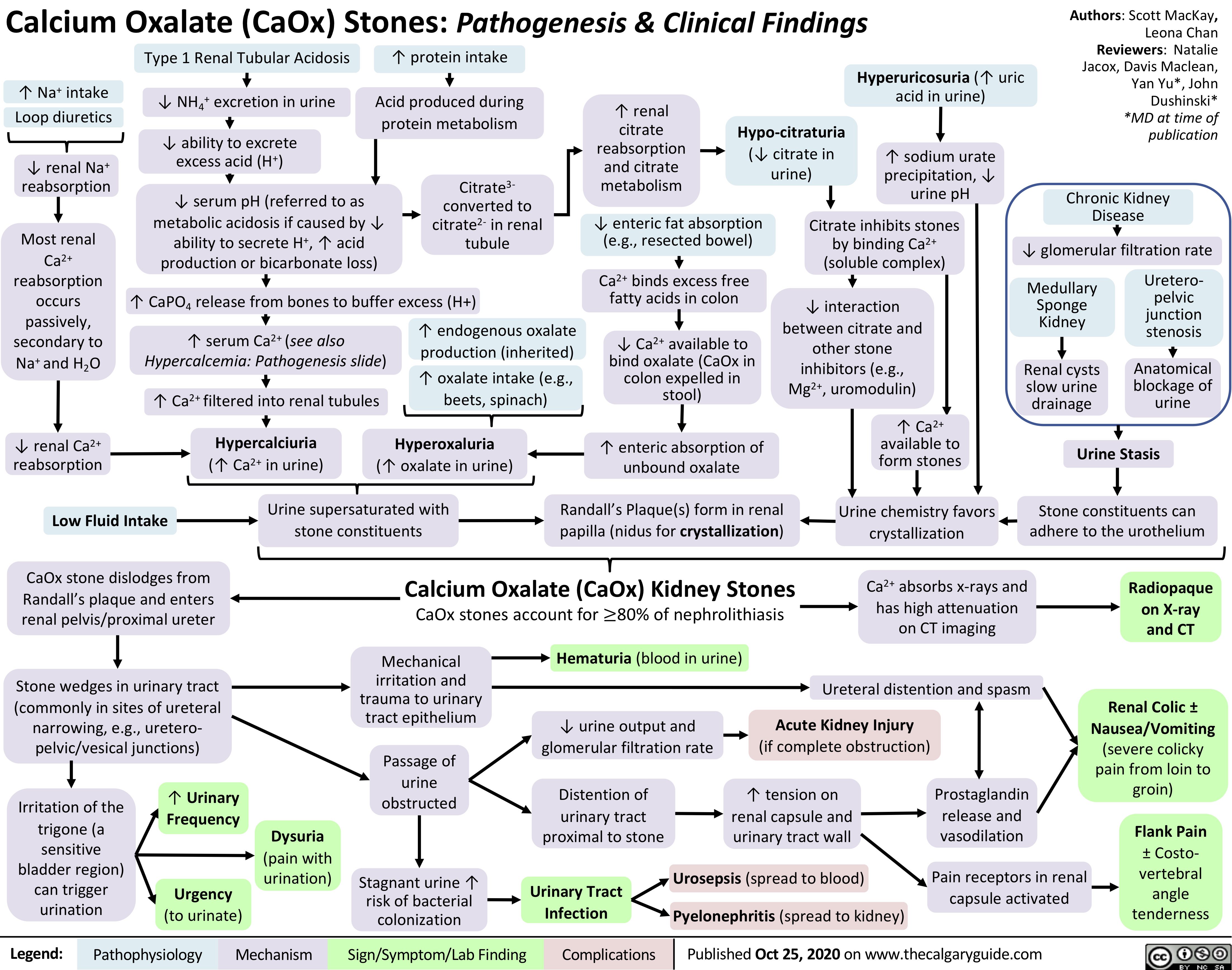
Calcium-Oxalate-Kidney-Stones
generalized-absence-seizures-petit-mal
 Seizure Hyperventilation: A common trigger of absence seizures
in pediatric patients with existing absence seizures ↑ respirationà↑ CO2 expelled from body & blood
↓ acidic CO2 levels in bloodà↑ blood pH (↓ blood acidity)
Predisposes neurons to fire spontaneously and asynchronouslyà↓ seizure threshold
Pathogenesis of absence seizure is complex and not yet fully elucidated, but evidence supports the cortical focus theory:
Hyperexcitable focal neurons on cerebral cortex send activation signals down to thalamocortical neuron network
Activated neurons in thalamus interact with cortical neurons to produce rhythmic oscillatory neuronal firing (brain waves) between these two regions of the brain
Abnormal rhythmic and bilaterally synchronous activation of the cerebral cortex during wakefulness
Between seizures (inter-ictal)
Inter-ictal changes in neuronal firing patterns and connectivity in sensorimotor cortices (mechanism unclear)
First degree relative with absence epilepsy
Genetic predisposition/idiopathic (>90%)
No single identified cause such as a structural lesion or single genetic mutation
Multiple gene mutations that predispose to epilepsy when occurring together
Authors: Alyssa Federico, Davis Maclean, Erika Russell, Harjot Atwal Reviewers: Ario Mirian, Shaily Singh*, Kim Smyth*, Yan Yu* * MD at time of publication
Monogenetic mutation (<10%)
Single gene mutation predisposing to epilepsy
Mutations involve genes encoding voltage-gated calcium channels and gamma aminobutyric acid (GABA) receptors, which are important in regulating thalamocortical activity
Absence Seizure:
Brief lapse of consciousness with a vacant stare lasting 3-10 seconds, without convulsions or loss of motor tone. May occur up to 100 times per day.
Seizure features (ictal phase)
Absence seizures generally occur in the context of an epilepsy syndrome and present in childhood
Childhood absence epilepsy: Most common form of pediatric epilepsy, characterized by absence seizures
Juvenile absence epilepsy:
Characterized by absence seizures +/- generalized tonic-clonic seizures
Juvenile myoclonic epilepsy:
Characterized by myoclonic seizures +/- absence seizures
Post-seizure (post-ictal)
Mechanisms unclear
Consciousness regained immediately after seizure
No post-ictal symptoms
No memory of event
Neuropsychiatric symptoms (poor attention, memory, mood, cognition) seen in 60% of children
Smooth/rapid transition to seizure
No aura (warning sign) prior to seizures
Seizure activity directly or indirectly impairs communication between neural networksà alters activity of brain structures involved in maintaining awareness
Some simple response to internal or external stimuli
may remain intact (mechanisms unclear)
Automatisms: Eye movements (fluttering), oral (lip smacking, swallowing, chewing), manual (finger tapping, scratching)
Brain wave oscillations generated in the thalamus
EEG findings: Generalized 3 Hz
spike-wave activity with maximum amplitude in both frontal lobes
Impaired awareness
Inhibition of
response to external stimuli
Impaired school performance and social interactions
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 2, 2021 on www.thecalgaryguide.com")
Lambert-Eaton-Myasthenic-Syndrome-Pathogenesis-and-Clinical-Findings
 in >50% of patients
Tumour membrane expresses voltage-gated calcium channels (VGCCs), which normally exist on neurons and function in neurotransmission
Note:
A paraneoplastic syndrome is a condition that arises due to cancer elsewhere in the body; possibly an immune response against tumour cells
Positive anti-VGCC IgG on serology
↓ Stimulation of salivary glands à↓ production of saliva
↓ Nitric oxide & prostaglandin production by cavernosal endothelial cellsàImpaired vasodilation of penile arteries
↓ Acetylcholine-induced gastric motility
↓ Acetylcholine available to mediate muscle reflexes
↑ Variability in action potential initiation along muscle fibers
Immune response to foreign cancer cells triggers production of antibodies against VGCCs on the cell surfaces of presynaptic neurons
Antibodies bind VGCCs, blocking Ca2+ Antibodies bind, cross-link, and
from entering presynaptic neurons
↓ Ca2+ influx into the presynaptic neuron during its depolarization
internalize VGCCsà↓ VGCC on neuron surface
Xerostomia (dry mouth)
Erectile dysfunction
Constipation
↓ Deep tendon reflexes
Unstable motor unit action potentials on electromyography
↓ Baseline compound muscle action potentials (CMAPs:
summated action potentials of all motor endplates in one muscle) on nerve conduction studies
Since intracellular Ca2+ mediates neurotransmitter vesicle fusion with the presynaptic membrane, ↓ Ca2+ influx ↓release of neurotransmitters like acetylcholine into the synaptic cleft
However, with repeated stimulation of the presynaptic neuron (e.g. exercise), there is ↑ Ca2+ accumulation within the axon terminal, allowing for more neurotransmitter vesicle fusion with the presynaptic membrane
↑ Acetylcholine available to mediate muscle reflexes
With high frequency repetitive nerve stimulation, ↑ number of compound CMAPS can be generated
↓ Acetylcholine release into synapses leading to autonomic nerves
↓ Acetylcholine release into neuromuscular junction
Autonomic dysfunction
↑ Deep tendon reflex amplitude
Temporary improvement in muscle strength
↓ Number of
muscle fibers activated by each action potential
Post-activation facilitation: Repeated stimulation improves symptoms
Larger proximal muscles involved in movement (i.e. walking) do not recruit sufficient number of muscle fibers for proper function
Can affect any muscle group, but muscles involved in speech, swallowing, and periocular muscles are often afflicted
Gait disturbance
Symmetric skeletal muscle weakness
Dysarthria (difficulty speaking)
Dysphagia (difficulty swallowing)
Ptosis (drooping of upper eyelid)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 18, 2021 on www.thecalgaryguide.com")
Hypercortisolemia
: Clinical Findings
Cortisol is a net catabolic hormone affecting many body systems, serving to release energy into the blood in response to stress. Excess cortisol also impacts circulation and impairs immune function. Excess Serum Cortisol affects:
Authors: Samin Dolatabadi, Yan Yu* Reviewers: Meena Assad, Amanda Henderson, Brooke Fallis, David Campbell* * MD at time of publication
Bone and Calcium Metabolism
Kidney and vasculature
Excess cortisol in the renal tubule saturates the enzyme 11β- HSD2, which converts cortisol to cortisone
Capacity of body to convert cortisol to cortisone is exceeded
Excess cortisol can mimic aldosterone
and bind to mineralocorticoid receptors (cortisone can’t bind to these receptors)
↑ Aldosterone effect → ↑ Na+ reabsorption from the cortical collecting duct into blood vessels
Liver and Peripheral Tissue
Cortisol ↑ gluco- neogenesis in liver, and ↑ insulin resistance by body tissue (unclear mechanisms)
Hyper- glycemia
Reproductive System
Cortisol exerts negative feedback on hypothalamus
à↓ gonadotropin releasing hormone (GnRH) secretion
↓ GnRH → ↓ LH/FSH → ↓ estrogen and testosterone production (especially important in females)
Infertility, ↓ Libido, Irregular Menses
Adipose Tissue
Cortisol ↑ fat breakdown (lipolysis)
Selective expression of cortisol receptor on different adipose tissuesàcentral, facial, dorsal fat is less broken down than in other areas (mechanism unclear)
Combined with cortisol ↑ appetite:
Skin & Connective Tissue
↑ Serum cortisol à↓ Fibroblast proliferation → ↓ Collagen synthesis
Skin atrophy with loss of connective tissue
Muscle
↑ Proteolysis & ↓ Protein synthesisà↓ muscle growth and function
Immune System
Normal serum cortisol protects against damaging effects of uncontrolled inflammatory and immune responses
↑ Serum cortisolà over-suppression of inflammation and impaired cell- mediated immunity
↑ Serum cortisol leads to ↓ Intestinal Ca2+ absorption and ↓ renal Ca2+ reabsorption
↓ Serum Ca2+ ↑ PTH secretion
↑ Serum cortisolà↑ RANKL:OPG ratio
↓ Osteoblast activity & ↑ Osteoclast activity
Cardiac muscle
Cardio- myopathy, Heart Failure
Skeletal
muscle, especially upper arms & thighs (for unclear reasons)
Proximal Muscle Weakness
Easy Bruising
↑ abdominal size stretches the fragile skin to become thinneràvenous blood of the underlying dermis becomes visible
Purple Striae
If hypertension is chronic
Ca2+ resorption from bone into the blood
Osteoporosis
Supraclavicular & Dorsal Fat Pads
Central Obesity
Poor Wound Healing
Susceptibility to infection
Round Face (Moon Face)
Abbreviations:
• RANKL – Receptor activator of nuclear factor kappa-Β ligand • OPG – Osteoprotegerin
• 11β-HSD2 – 11β-hydroxysteroid dehydrogenase type 2
Water follows Na+ into blood vessels to balance the osmotic pressure between the blood and renal tubules
Water reabsorption → Expansion of blood volume
Hypertension
Both primary Cushing’s (e.g. adenomas that extend into zona reticularis of the adrenal cortex) and central/secondary Cushing’s (e.g. ↑ ACTH stimulation of zona reticularis) are associated with ↑ adrenal androgen secretion
Removal of positively charged Na+ from tubular lumen creates a negative luminal environment
K+ follows the electrical gradient and is secreted into tubular lumen
↓ Serum K+ concentration
Hypokalemia
Arrhythmia, Paralysis, Cramps
(see Hypokalemia: Clinical Findings slide)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 17, 2021 on www.thecalgaryguide.com
Hirsutism, Acne")
Overview of Calcium Phosphate Vitamin D Physiology
 and ↓ expression of osteoprotegerin (OPG), a decoy receptor for RANKL
RANKL binds to receptor activator of nuclear factor kappa-B (RANK) on osteoclasts
↑ Osteoclast differentiation and activity
↑ Ca2+ resorption from bone into blood
Sensed by Calcium-Sensing Receptor on Chief Cells of the Parathyroid Gland
− −
↑ Serum phosphate (PO4) ↓ Serum calcium (Ca2+)
Parathyroid Gland releases Parathyroid Hormone (PTH) into the blood, which acts on the kidneys and the bones
Kidney
↑ Activation of Transient Receptor Potential Vanilloid subfamily member 5 (Ca2+ channel)
in the distal convoluted tubule
↓ Expression of 24-hydroxylase enzyme (which functions to catabolize calcitriol)
↑ Expression of 1α- hydroxylase enzyme
↑ Conversion of 25-hydroxy vitamin D (Calcidiol) to the
active form, 1,25-dihydroxy vitamin D (Calcitriol)
↑ Calcitriol Small Intestine
↑ Endocytosis of sodium phosphate co-transporters NaPi-2a and NaPi-2c, which reabsorb PO4 from ultrafiltrate in the renal tubules
↓ Reabsorption of PO 4
↓ Serum PO
Calcitriol negatively feeds back on parathyroid gland to inhibit PTH production
↑ Expression of sodium phosphate co- transporters NaPi-2a and NaPi-2b that absorb PO4 from intestinal lumen
4
↑ Expression of apical epithelial Ca2+ channels (Transient Receptor Potential Vanilloid subfamily member 6)
↑ Entry of Ca2+ on apical side of enterocytes
↑ Reabsorption of Ca2+ in the distal convoluted tubule through Ca2+ channels
↑ Reabsorption of PO
↑ Expression of cytoplasmic Calbindin-D
↑ Transport of Ca2+ across enterocytes
↑ Absorption of Ca2+ in small intestine
↑ Serum Ca+2
↑ Expression of basolateral plasma membrane calcium ATPase
↑ Extrusion of Ca2+ from enterocytes into bloodstream
4
Authors: Samin Dolatabadi, Hannah Yaphe Reviewers: Amanda Henderson, Meena Assad, Brooke Fallis, Yan Yu*, Hanan Bassyouni* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
First published Oct 15, 2017, updated Nov 11, 2021 on www.thecalgaryguide.com")
complications-of-chronic-kidney-disease-ckd

Authors: Samin Dolatabadi, Brooke Fallis Reviewers: Jessica Krahn, Meena Assad, Yan Yu* Juliya Hemmett* * MD at time of publication
Abnormalities of kidney structure or function that is present for 3 or more months
Kidney tubules atrophy & kidney interstitial tissue undergo fibrosis
Kidney damage ↓ erythropoietin production (normally a kidney function)
↓stimulation of bone marrow → ↓ red blood cell production
Build up of toxic substances (e.g. urea, guanidine, and indoxyl sulfate)
↓ Conversion of calcidiol to calcitriol in by kidney
↓ Calcitriol levels in blood
↓ Ca+2 absorption from small intestine
Hypocalcemia
↓ Glomerular Filtration Rate
↑ Vascular calcification and endothelial dysfunction (e.g. changes in permeability, clotting response to inflammation, amongst other mechanisms)
Atherosclerotic disease (see “Complications of Atherosclerosis” slide)
↓ Lipoprotein lipase, apoA-1, and Lecithin-cholesterol acyltransferase
activity acting on serum lipoproteins (complex mechanisms)
↓ Lipoprotein clearance from blood
Dyslipidemia (↑ LDL, ↑ triglycerides, ↓ HDL)
Toxic damage ↓ red blood cell survival
Anemia
Uremic Syndrome
↓ Renal excretion of phosphate
↑ phosphate remaining in bloodstream
Hyperphosphatemia
↑ serum phosphate binds with ionized calcium
↓ Renal excretion of K+
↑ K+ remaining in bloodstream
Hyperkalemia Edema
↓ Renal excretion of ammonium
Reduced filtration capability ↑ organic anions remaining in blood→ ↑ anion gap
↓ Renal excretion of salt and water
↑ in extracellular fluid → systemic volume overload
↓ calcium in blood ↓ inhibition of Parathyroid Hormone (PTH) release
↑ PTH in blood
Secondary hyperparathyroidism
Metabolic Acidosis
Hypertension
Pitting
Chronic kidney disease – mineral and bone disorder (CKD-MBD)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 4, 2022 on www.thecalgaryguide.com")
induction-of-labour-ripening-of-the-cervix-mechanisms-and-methods

Please refer to “Induction of labour: Indications and contraindications” slide
Bishop Score > 6
Cervix favorable
↑ Natural release of prostaglandins from uterine wall
Bishop Score 4-5
Proceed based on clinical picture
Amniotic membranes intact
Amniotomy to artificially rupture amniotic membranes
Rush of amniotic fluid
Bishop Score < 3
Cervix unfavorable and requires ripening
Artificial prostaglandin into vagina (gel or vaginal insert)
Ripening options
Ripening balloon in cervix
Pressure applied to internal and external cervical os
Foley catheter in cervix
Pressure applied to internal cervical os
Act as calcium ionophores to áintracellular Ca2+
Activate EP1 and EP3 receptors on myometrial cells
Lack of fluid cushion causes more fetal head engagement
Fluid flow may carry umbilical cord with it
Cord prolapse (if fetal head not engaged/ low enough in pelvis to block exit of cord)
Degradation of
collagen in the connective tissue stroma of cervix
Cervix softens
Cervical dilation
Cervix stretches (until balloon falls out)
Author: Lindey Felske Reviewers: Ran (Marissa) Zhang Brianna Ghali Ingrid Kristensen* * MD at time of publication
Risk of uterine rupture
(if prostaglandins used as a ripening method after previous C- section)
Uterine contractions
↑ Myometrial contractility
↑ Pressure on cervix
Labour
If needed, proceed to amniotomy and/or oxytocin once cervix is favorable
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 4, 2022 on www.thecalgaryguide.com")
presentation-of-sah
![Subarachnoid Hemorrhage: Clinical Findings
Sudden bleeding into space surrounding the brain (for pathogenesis, see Subarachnoid Hemorrhage: Pathogenesis)
Authors: Jason An, M. Patrick Pankow Reviewers: Owen Stechishin, Dave Nicholl, Haotian Wang, Hannah Mathew, Ran (Marissa) Zhang, Yan Yu*, Cory Toth* * MD at time of publication
Bleed into subarachnoid space
Subarachnoid Hemorrhage (SAH)
Posterior hypothalamus ischemia (↓ Blood flow and oxygen)
Red blood cell lysis from energy depletion or complement activation
Release of spasmogens (spasm inducing agents)
Cerebral vasospasm (narrowing of arteries from persistent contraction) ↓ blood flow
Cerebral ischemia
Release catecholamines (hormones from the adrenal gland; e.g., epinephrine, norepinephrine)
↑ Intracellular calcium
Release of antidiuretic hormone
Antidiuretic hormone acts on the distal convoluted tubule and collecting duct in kidney to reabsorb water
Dilution of serum sodium
Hyponatremia (low blood sodium levels)
Release of epileptogenic (potential seizure causing agents) into cerebral circulation
Seizure
Products from blood breakdown in cerebral spinal fluid
Irritation of meninges (membranes surrounding the brain)
Aseptic meningitis (non-infectious inflammation)
Meningismus
(neck pain + rigidity)
Cerebral infarction (death of tissue)
Obstructs cerebral spinal fluid flow and absorption at subarachnoid granulations
Hydrocephalus (fluid build up in ventricles)
↓ Level of consciousness
Reduced cerebral blood flow
Dilation of cranial vessels to ↑ blood flow
Rapid ↑ internal carotid artery intracranial pressure
Refer to Increased Intracranial Pressure: Clinical Findings slide
Internal carotid artery
Pituitary ischemia
Hypopituitarism
[underactive pituitary gland, failing to produce 1+ pituitary hormone(s)]
Refer to hypopituitarism slides
Myocardial disruption
Left ventricle dysfunction
↑ Pressure in left heart
Blood forced backwards into pulmonary veins
↑ Pulmonary blood pressure
Fluid from blood vessels leaks into lungs
Dysrhythmias (disturbance in rate/rhythm of heart) causing ↓ cardiac output
Syncope
(loss of consciousness due to ↓ blood flow to the brain)
Pulmonary edema
(excess accumulation of fluid in lung)
Cerebral hypoperfusion
Sudden ↑in blood volume
Vessels and meninges suddenly stretch
Thunderclap Headache (worst headache of patient's life)
Shortness of breath
Reactive cerebral hyperemia (excess blood in vessels supplying the brain)
Artery specific findings:
Rapid ↑ internal carotid artery intracranial pressure
Middle cerebral artery
Posterior communicating artery
Compression of outer CN3 Compression of inner CN3
Anterior communicating artery
Nonreactive pupil
Gaze palsy
(eye deviates down and out)
Diplopia
(double vision)
Ptosis
(drooping of upper eyelid)
Frontal lobe ischemia
Avolition
(complete lack of motivation)
Ischemia of motor strip pertaining to the legs
Bilateral leg weakness
Motor strip ischemia
Hemiparesis
(weakness/ inability to move one side of the body)
Ischemia of parietal association areas (brain regions integral for motor control of the eyes, the extremities and spatial cognition)
Aphasia
(impaired ability to speak and/or understand language)/ neglect
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 1, 2014, updated August 10, 2022 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/SAH-Clinical-Findings-2022.jpg "Subarachnoid Hemorrhage: Clinical Findings
Sudden bleeding into space surrounding the brain (for pathogenesis, see Subarachnoid Hemorrhage: Pathogenesis)
Authors: Jason An, M. Patrick Pankow Reviewers: Owen Stechishin, Dave Nicholl, Haotian Wang, Hannah Mathew, Ran (Marissa) Zhang, Yan Yu*, Cory Toth* * MD at time of publication
Bleed into subarachnoid space
Subarachnoid Hemorrhage (SAH)
Posterior hypothalamus ischemia (↓ Blood flow and oxygen)
Red blood cell lysis from energy depletion or complement activation
Release of spasmogens (spasm inducing agents)
Cerebral vasospasm (narrowing of arteries from persistent contraction) ↓ blood flow
Cerebral ischemia
Release catecholamines (hormones from the adrenal gland; e.g., epinephrine, norepinephrine)
↑ Intracellular calcium
Release of antidiuretic hormone
Antidiuretic hormone acts on the distal convoluted tubule and collecting duct in kidney to reabsorb water
Dilution of serum sodium
Hyponatremia (low blood sodium levels)
Release of epileptogenic (potential seizure causing agents) into cerebral circulation
Seizure
Products from blood breakdown in cerebral spinal fluid
Irritation of meninges (membranes surrounding the brain)
Aseptic meningitis (non-infectious inflammation)
Meningismus
(neck pain + rigidity)
Cerebral infarction (death of tissue)
Obstructs cerebral spinal fluid flow and absorption at subarachnoid granulations
Hydrocephalus (fluid build up in ventricles)
↓ Level of consciousness
Reduced cerebral blood flow
Dilation of cranial vessels to ↑ blood flow
Rapid ↑ internal carotid artery intracranial pressure
Refer to Increased Intracranial Pressure: Clinical Findings slide
Internal carotid artery
Pituitary ischemia
Hypopituitarism
[underactive pituitary gland, failing to produce 1+ pituitary hormone(s)]
Refer to hypopituitarism slides
Myocardial disruption
Left ventricle dysfunction
↑ Pressure in left heart
Blood forced backwards into pulmonary veins
↑ Pulmonary blood pressure
Fluid from blood vessels leaks into lungs
Dysrhythmias (disturbance in rate/rhythm of heart) causing ↓ cardiac output
Syncope
(loss of consciousness due to ↓ blood flow to the brain)
Pulmonary edema
(excess accumulation of fluid in lung)
Cerebral hypoperfusion
Sudden ↑in blood volume
Vessels and meninges suddenly stretch
Thunderclap Headache (worst headache of patient's life)
Shortness of breath
Reactive cerebral hyperemia (excess blood in vessels supplying the brain)
Artery specific findings:
Rapid ↑ internal carotid artery intracranial pressure
Middle cerebral artery
Posterior communicating artery
Compression of outer CN3 Compression of inner CN3
Anterior communicating artery
Nonreactive pupil
Gaze palsy
(eye deviates down and out)
Diplopia
(double vision)
Ptosis
(drooping of upper eyelid)
Frontal lobe ischemia
Avolition
(complete lack of motivation)
Ischemia of motor strip pertaining to the legs
Bilateral leg weakness
Motor strip ischemia
Hemiparesis
(weakness/ inability to move one side of the body)
Ischemia of parietal association areas (brain regions integral for motor control of the eyes, the extremities and spatial cognition)
Aphasia
(impaired ability to speak and/or understand language)/ neglect
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 1, 2014, updated August 10, 2022 on www.thecalgaryguide.com")
diabetes-insipidus-pathogenesis-and-clinical-findings
![Diabetes Insipidus: Pathogenesis and clinical findings
Hereditary
Autoimmune/ Idiopathic
Auto-antibodies destroy neurons that release antidiuretic hormone (ADH)
Mass Effect/ Tumor Invasion
Mass pressing on hypothalamus or pituitary
Electrolyte Imbalance
(mechanism unclear)
Hereditary
Lithium (Li)
(mechanism unclear)
Li enters principal cells of collecting ducts via ENaCs
Li inhibits GSK3β, reducing adenylyl cyclase activity
↓ cAMP- dependent phosphorylation of aquaporin-2
↑ Serum [Ca2+]
Activation of
CaSR in thick ascending limb of Loop of Henle
↓ NaCl reabsorption in thick ascending limb
↓ Generation of medullary osmotic gradient
↓ Serum [K+]
↑ Degradation of aquaporin-2 channels in collecting duct
↓ Aquaporin- 2 channels transporting water across apical membrane of collecting duct
Mutation of AVPR2 gene on X chromosome
Antidiuretic hormone (ADH) receptor cannot reach basolateral surface of principal cells of collecting duct
Mutation of aquaporin-2 gene on chromosome 12
↓ Fusion of aquaporins with apical membrane of collecting duct
Mutation of WFS1 gene on chromosome 4 (Wolfram syndrome)
↓ Processing of antidiuretic hormone (ADH) precursors and ↓ADH-releasing neurons
Surgery/ Trauma
Injury to hypothalamus or pituitary stalk
Mutation of PCSK1 gene on chromosome 5
Deficiency in PC1/3 (encoded by PCSK1)
↓ Processing of ADH by PC1/3
Aquaporin dysfunction
↓ Kidney response to ADH, which mediates reabsorption of water down its osmotic gradient through aquaporins
↓ Production of ADH by hypothalamus or ↓ secretion from ADH-releasing neurons in posterior pituitary (depending on location of lesion)
Central Diabetes Insipidus
Nephrogenic Diabetes Insipidus
Abbreviations:
AVPR2: arginine vasopressin receptor 2 CaSR: calcium-sensing receptor
ENaC: epithelial sodium channel
GSK3β: glycogen synthase kinase type 3 beta PC1/3: proprotein convertase
Diabetes Insipidus
Decreased ability of kidneys to concentrate urine
↓ Reabsorption of water from collecting duct into vasculature
Author:
Oswald Chen
Reviewers:
Huneza Nadeem,
Ran (Marissa) Zhang,
Yan Yu*
Sam Fineblit*
* MD at time of publication
Urine becomes more dilute
↓ Urine osmolality
↑ Urine output
↓ Blood volume
Blood becomes more concentrated
Occurs during late sleep period
Nocturia
Polyuria
(>3 L/day)
↑ Serum osmolality
Activation of hypothalamic osmoreceptors
Hypernatremia
(Serum [Na+] >145 mEq/L)
Polydipsia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 25, 2022 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2022/09/Diabetes-Insipidus.jpg "Diabetes Insipidus: Pathogenesis and clinical findings
Hereditary
Autoimmune/ Idiopathic
Auto-antibodies destroy neurons that release antidiuretic hormone (ADH)
Mass Effect/ Tumor Invasion
Mass pressing on hypothalamus or pituitary
Electrolyte Imbalance
(mechanism unclear)
Hereditary
Lithium (Li)
(mechanism unclear)
Li enters principal cells of collecting ducts via ENaCs
Li inhibits GSK3β, reducing adenylyl cyclase activity
↓ cAMP- dependent phosphorylation of aquaporin-2
↑ Serum [Ca2+]
Activation of
CaSR in thick ascending limb of Loop of Henle
↓ NaCl reabsorption in thick ascending limb
↓ Generation of medullary osmotic gradient
↓ Serum [K+]
↑ Degradation of aquaporin-2 channels in collecting duct
↓ Aquaporin- 2 channels transporting water across apical membrane of collecting duct
Mutation of AVPR2 gene on X chromosome
Antidiuretic hormone (ADH) receptor cannot reach basolateral surface of principal cells of collecting duct
Mutation of aquaporin-2 gene on chromosome 12
↓ Fusion of aquaporins with apical membrane of collecting duct
Mutation of WFS1 gene on chromosome 4 (Wolfram syndrome)
↓ Processing of antidiuretic hormone (ADH) precursors and ↓ADH-releasing neurons
Surgery/ Trauma
Injury to hypothalamus or pituitary stalk
Mutation of PCSK1 gene on chromosome 5
Deficiency in PC1/3 (encoded by PCSK1)
↓ Processing of ADH by PC1/3
Aquaporin dysfunction
↓ Kidney response to ADH, which mediates reabsorption of water down its osmotic gradient through aquaporins
↓ Production of ADH by hypothalamus or ↓ secretion from ADH-releasing neurons in posterior pituitary (depending on location of lesion)
Central Diabetes Insipidus
Nephrogenic Diabetes Insipidus
Abbreviations:
AVPR2: arginine vasopressin receptor 2 CaSR: calcium-sensing receptor
ENaC: epithelial sodium channel
GSK3β: glycogen synthase kinase type 3 beta PC1/3: proprotein convertase
Diabetes Insipidus
Decreased ability of kidneys to concentrate urine
↓ Reabsorption of water from collecting duct into vasculature
Author:
Oswald Chen
Reviewers:
Huneza Nadeem,
Ran (Marissa) Zhang,
Yan Yu*
Sam Fineblit*
* MD at time of publication
Urine becomes more dilute
↓ Urine osmolality
↑ Urine output
↓ Blood volume
Blood becomes more concentrated
Occurs during late sleep period
Nocturia
Polyuria
(>3 L/day)
↑ Serum osmolality
Activation of hypothalamic osmoreceptors
Hypernatremia
(Serum [Na+] >145 mEq/L)
Polydipsia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 25, 2022 on www.thecalgaryguide.com")
Pubic Rami Fracture: Pathogenesis and clinical findings

Bone loses calcium, becoming less dense weaker and more susceptible to fracture (See Osteoporosis: pathogenesis and clinical findings slide)
Athletic injury in skeletally immature athletes (e.g., soccer, gymnastics)
Open growth plates are weak and more susceptible to injury
Lateral compression or vertical shear fracture
Mild to moderate osteoporosis
Fragility pubic rami fracture from low-energy impact (e.g., falls from standing, falls in the bathtub)
Severe osteoporosis
Spontaneous pubic rami fracture
Sudden, forceful contraction of the hamstring muscles (e.g. sudden change of direction, sudden stop)
Hamstring pulls a piece of the ischial tuberosity from the pelvis boneàpubic rami avulsion fracture
(Posterior pelvic rim fracture
requires CT to diagnose and is often missed)
Missed or delayed diagnosis due to incomplete workup
Pubic Rami Fracture
Fracture of the anterior pelvic ring, can be the superior and/or inferior pubic rami
Co-existing posterior pelvic ring fracture (e.g. acetabulum, sacrum)
Fracture on both sides of pelvis
Unstable pelvis
Blood vessels in and surrounding the bone rupture during injury
Blood accumulates under the skin
Bruising around fracture site
Inflammatory response to injury
Recruitment of white blood cells and fluid to the area
Swelling around fracture site
Irritation at superior/inferior pubic rami muscle attachment sites (groin and hip abductor muscles)
Pain in groin near fracture site
↑ Displacement and incomplete healing of the posterior and anterior pelvic ring fracture
↑ Morbidity and mortality
↑ Disuse osteoporosis ex: lower limbs, pelvis, and back
↑ Muscle stiffness ex: lower limbs, pelvis, and back
↑ Joint stiffness ex: lower limbs, pelvis, and back
Fracture hematoma in pubic rami
Hematoma distends the periosteum, irritating nerves in the area
Moving/walking further irritates nerves in the area
Moving and walking ↑ pain àinadequate movement
↓ Mobility (to avoid pain)
Antalgic gait (stance phase of walking is shortened relative to swing phase)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 4, 2022 on www.thecalgaryguide.com")
Concussion

Disruption of reticular activating system (brain area that regulates arousal)
Altered level of consciousness
Direct blow to the head or the body that causes an impulsive force to the head (i.e., falls, motor vehicle accidents, sports, assaults)
Skull acceleration / deceleration
Coup (brain strikes skull on side of impact)
Brain tissue swelling
Cerebral edema (fluid build up around brain)
↑ Intracranial pressure
Cerebral herniation
(shifting of brain tissue into adjacent space)
Contrecoup (brain strikes skull on opposite side of impact)
Anatomical damage
Skull fracture
Broken bone fragments ruptures blood vessels
Intracranial hemorrhage
(bleeding into brain tissue)
Papilledema (swelling around optic disk, where optic nerve enters eyeball)
Disruption of messages from eye to brain
Vision problems (i.e., blurred or double vision)
Cellular damage
Indiscriminate, rapid neurotransmitter release
↑Extracellular K+ and glutamate, accumulation of intracellular calcium
Ionic disequilibrium across neuronal membrane
Energy consumed by Na+/K+ ATPase pumps to re-establish ionic homeostasis
↑ Cerebral glucose metabolism
↑ Energy demand
Brain injury
Axonal stretch due to
biomechanical forces
Microtubule disruption
Structural (cytoskeletal) disturbance
Axonal degeneration
Impaired neural communication
Broken bone fragments
Ruptures blood vessels
Compresses blood vessels
↓ Cerebral blood flow
↓ Cerebral glucose supply
↓ Energy supply
↓ Oxygenated blood to brain
Brain cell death
Chronic brain atrophy
Persistent impaired cognition
Cellular energy crisis (mismatch between energy supply and demand due to effort in restoring homeostasis)
Nausea, vomiting
↓ Participation in daily Confusion, disorientation, unsteadiness, headache activities and work
Death Anxiety, depression
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 12, 2019, updated March 27, 2023 on www.thecalgaryguide.com")
Carpal Tunnel Syndrome

↑ Blood sugar: deposition of advanced glycation end (AGE) products (proteins or lipids glycated when exposed to sugar)
AGE attaches to and prevents tendons from moving properly
Authors: Amanda Eslinger Yvette Ysabel Yao Reviewers: Matthew Harding Owen Stechishin Mao Ding, Cory Toth* * MD at time of publication
Wrist trauma (distal radius fractures, carpal/metacarpal fractures, tendon ruptures)
Repetitive Strain Injury (repetitive hand & wrist movements)
Irritation, swelling & thickening of tendons in carpal tunnel
Calcium deposits
Calcifica tion
Deposition Amyloidosis
Amyloid
(protein aggregates) deposition
Gout
(See Gout Slide)
Uric acid crystal deposition
Pregnancy
↑ Concentration of hormones & uterine pressure on inferior vena cava
Backup of blood into systemic circulation
Autoimmune
(i.e. Rheumatoid arthritis, scleroderma, lupus, Sjogren’s syndrome)
↑ Inflammatory cytokines causing inflammation
Hypo- thyroidism
Myxedema (swelling of skin and underlying tissues) in carpal tunnel
Idiopathic or Congenital
Edema
Narrowed carpal tunnel leads to ↑ internal pressure
Carpal Tunnel Syndrome
Vascular: median artery thrombosis in carpal tunnel
Median nerve compression inside the carpal tunnel Mechanical disruption of median nerve
Compression exacerbated with flexed wrists (i.e. sleep, driving, holding phone/cup)
Disruption of daily activities and sleep
Ischemia (↓ blood supply) to median nerve
Hypoxia (↓ oxygenated blood flow)
Metabolic conduction block (impaired axonal transport due to ischemia)
Nerve conduction study
(show sensory nerve impulses slowing across the wrist, followed by mild / moderate / severe loss of sensory nerve amplitude
Damage to the myelin sheath
↓ Saltatory conduction (action potential propagation along myelinated axons)
Neuropraxia (nerve compression blocks conduction)
Interruption in axonal continuity
Axonotmesis (endoneural tube stays intact but myelin & distal axon degenerates)
Recovery possible
Full disruption of myelin, axon & nerve sheath
Neurotmesis (axons no longer have an endoneural tube to guide regrowth)
Recovery impossible
↓ Ability to contract and use abductor pollicis brevis muscle
↓ Signals through median nerve
Interference with signals to the brain causes unusual sensations
Hypoalgesia (↓ pain Dysesthesia (tingling, burning, or sensitivity at 1st 3 1⁄2 digits) painful sensation at 1st 3 1⁄2 digits)
Thenar muscle wasting
Reduced hand dexterity
Weak thumb abduction
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 2nd, 2013, updated March 22, 2023 on www.thecalgaryguide.com")
Physiology of Anti-diuretic hormone
/Arginine Vasopressin (AVP)
Authors: Manaswi Yerrabattini Reviewers: Parker Lieb Mao Ding Shyla Bharadia Laura Hinz* * MD at time of publication
Limbic activation (e.g., pain, nausea)
Placental production of vasopressinase during pregnancy catalyzes the breakdown of ADH, leading to a temporary Diabetes Insipidus state (see Diabetes Insipidus: Pathogenesis and Clinical Findings slide)
Systemic arteriole vasoconstriction
Hypovolemia/Hypotension
Hyperosmolar state (i.e., extracellular fluid osmolarity above a certain threshold, most commonly due to hypernatremia)
Sensed by osmoreceptors in hypothalamus
Angiotensin II synthesized through activation of Renin- Angiotensin-Aldosterone System (RAAS) (see Physiology of RAAS slide)
Binds to receptors located in the hypothalamus
↓ pressure sensed by baroreceptors in the heart (left atrium and large veins)
Receptors transmit signals to brain via the vagus nerve
↓ Arterial baroreceptor firing
↑ Sympathetic activity of nerves innervating afferent arterioles
↑ Hypothalamic secretion of ADH (peptide hormone), transportation to posterior pituitary, and release from posterior pituitary into blood circulation
Blood Vessels (Minor role)
Kidneys (Main role)
ADH binds to to Vasopressin-2 receptors on basolateral side of principal cells in kidneys
↑ Insertion of aquaporin II channels onto apical membrane of late distal tubule and collecting ducts
↑ Water reabsorption
↓ Urine Output and Maintains narrow range of serum osmolarity ↑ Urine Osmolarity and preserves sodium homeostasis
ADH binds to Vasopressin-1 receptors on smooth muscle of blood vessels
ADH activates calcium signaling pathway
↑ Blood Pressure
Maintains overall fluid volume status
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 20, 2023 on www.thecalgaryguide.com")
Sustained Monomorphic Ventricular Tachycardia Pathogenesis
 A ventricular scar forms (in the setting of coronary artery disease or cardiomyopathy) that cannot conduct electrical activity
The scar is surrounded by a circular conduction pathway consisting of an ⍺- limb (slow conduction with a fast refractory period) and a β-limb (fast conduction but a slow refractory period)
A correctly timed depolarization impulse arrives during the refractory period of the β-limb so it can only propagate through the ⍺-limb
The β-limb’s refractory period ends just before the impulse leaves the ⍺-limb of the circular pathway
Retrograde depolarization occurs into the ⍺ -limb, creating a self-sustaining closed- loop circuit within the ventricle
“Re-entry” cause of tachyarrhythmia
Idiopathic Causes: (10% of cases) Structurally normal heart on imaging
Trigger(s) such as catecholamines ↑ cyclic adenosine monophosphate
Intracellular calcium overload occurs in some ventricular myocytes
↑ Intracellular calcium activates sodium- calcium exchangers
Sodium influx into the myocytes
During normal myocyte repolarization, the net calcium-mediated depolarization reaches the myocyte threshold for an action potential
A triggered action potential (termed a “delayed afterdepolarization”) repeatedly occurs within the ventricle
“Triggered activity” cause of tachyarrhythmia
Authors:
Rahim Kanji
Reviewers:
Stephanie Happ, Raafi Ali, Derek Chew*
* MD at time of publication
Sustained Monomorphic Ventricular Tachycardia
A wide QRS complex tachycardia originating from the ventricles lasting > 30 seconds. Common
mechanisms include re-entry (e.g., scar-mediated) or a ventricular ectopic focus with increased automaticity. Refer to Sustained Monomorphic Ventricular Tachycardia: Clinical findings for details
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 22, 2023 on www.thecalgaryguide.com")
Carbonic Anhydrase Inhibitor Diuretics

Inhibition of carbonic anhydrase on the apical surface of the brush border cells in the proximal convoluted tubule (PCT)
Activation of the Renin- Angiotensin-Aldosterone Systemfromvolume depletion
Activation of principle cell
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+ and waste K+
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical
Findings slide
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H2O available for excretion
Mild diuresis (increase in frequencyandvolumeof urine)
↓ Blood volume
Hypotension
↓ Na+ and HCO3- reabsorption in the PCT
↑ HCO3- delivery to cortical collecting duct
Urine alkalization (increased pH)
Chronic urine alkalization
↓Solubilityof citrate
↓ Urinary citrate
↓ Citrate binding with Ca2+à↑ Ca2+ complexing with oxalate
↑ Spontaneous nucleation, growth and agglomeration of calcium oxalate crystals
Formation of calcium oxalate renal calculi
↑ HCO3- is lost in the urine ↓ pH of the blood
Type II Renal Tubular Acidosis
See Type II/Proximal Renal Tubular Acidosis slide
CAI prevents the up- regulationofglutamine transporters in the PCT
Inability to correct the metabolic acidosis and impaired urinary NH3 excretion
Hyperammonemia (↑ serum NH3 )
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 3, 2024 on www.thecalgaryguide.com
Carbonic Anhydrase Inhibitor Diuretics: Renal Mechanism and Side Effects Carbonic Anhydrase Inhibitors (CAI)
Inhibition of carbonic anhydrase on the apical surface of the brush border cells of the proximal convoluted tubule (PCT)
Authors: Stephanie Happ Reviewers: Matt Hobart Name Name* * MD at time of publication
↓ Na+ and HCO3- reabsorption in the PCT
↑ Na+ delivery to the cortical collecting duct (CCD)
H2O follows Na+ into the CCD to maintain a balanced osmotic pressure
↑ H O available for 2
excretion
Mild diuresis
↓ Blood volume Hypotension
↑ HCO3- delivery to cortical collecting duct
Epithelial sodium channels (ENaC) on principal cells of the CCD reabsorb ↑ Na+
↑ Intracellular Na+ drives Na+/K+ ATPase activity on the principal cells (moving 2 K+ into cell and 3 Na+ out into the peritubular capillary)
↑ Intracellular K+ drives H+/K+ ATPase activity on the intercalated cells (moving 1 H+ into cell and 1 K+ out into the tubular filtrate)
↓ K+ in serum
Hypokalemia
See Hypokalemia: Clinical Findings slide
Urine alkalization
↑ HCO3- is lost in the urine, leading to ↓ pH of the blood
Renal Tubular Acidosis Type II
See Type II/Proximal Renal Tubular Acidosis slide
CAI inhibit the up-regulation of glutamine transporters in the PCT
Inability to correct the metabolic acidosis and
impaired urinary NH3 excretion
Hyperammonemia
↑ Risk of hepatic encephalopathy in individuals with cirrhosis
Chronic urine alkalization leads to marked ↓ in urinary citrate
↓ Ability of citrate to bind to Ca2+ and calcium oxalate stones
↓ Inhibition of spontaneous nucleation
↓ Prevention of growth and agglomeration of crystals
Formation of calcium oxalate renal calculi
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published MONTH, DAY, YEAR on www.thecalgaryguide.com")
Dantrolene
, and spasticity associated with various neurological disorders such as multiple sclerosis, cerebral palsy, and spinal cord injury.
Dantrolene
Authors: Madison Amyotte, Arzina Jaffer Reviewers: Jasleen Brar, Mao Ding Luiza Radu Joanna Moser* * MD at time of publication
Metabolized in the liver by the cytochrome P450 enzyme
Metabolic process forms a high concentration of hydroxylamine
Hydroxylamine is a highly toxic metabolite associated with dantrolene induced liver injury
Impaired Liver Function
Binds to ryanodine receptors (RYR1) in the sarcoplasmic reticulum of skeletal muscle cells
Prevents ryanodine channel from opening when triggered by the action potential in the muscle
Prevents calcium release from the sarcoplasmic reticulum
Prevents binding of calcium to troponin on the actin filaments in the cytosol of the skeletal muscle cells
Myosin-binding site on the actin remains covered by the tropomyosin
Prevents cross-bridge formation between myosin and actin within the sarcomere
Prevents muscle contraction
↓ Progression of muscle rigidity and spasms ↓ Heat produced by muscular contraction
Skeletal & respiratory muscle weakness ↓ Body temperature
↓ Inspiratory capacity
Dyspnea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 18, 2024 on www.thecalgaryguide.com")
Metastatic Bone Lesions
 into bones. Once tumours metastasize to bone, they are generally incurable and contribute to significant morbidity prior to a patient’s death
Authors: Curtis Ostertag Reviewers: Mankirat Bhogal Nojan Mannani Michelle J. Chen Dr. Gerhard Kiefer* * MD at time of publication
Cell-to-cell communication between tumour cells & bone cells (osteoclasts & osteoblasts)
Tumours release TNF-⍺, RANK-L, and PTHRP which ↑ osteoclast activity & ↓ osteoblast activity
Change in relative activity of bone cells results in osteolysis (breakdown of bone)
Calcium is released into the bloodstream
Hypercalcemia
Osteoblastic metastasis (common in prostate cancer)
Tumor growth
Secondary bone formation in response to bone destruction
TGF-β, PDGF, & IGF are released from the degraded bone matrix, which can stimulate tumors & osteoblasts
Weakened bone increases risk of fracture
Pathologic fracture
↑ Mortality
Bone tissue expands into surrounding space
Nerve compression
Disruption of cortical bone or surrounding soft tissues
Diffuse & achy rest/night pain
Long bone masses compress peripheral nerves
Neuropathy
Vertebral masses compress spinal nerves/cord
Radiculopathy /Myelopathy
↓ Quality of life
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jun 9, 2024 on www.thecalgaryguide.com")
Massive Transfusion Protocol
![Massive Transfusion Protocol: Considerations and rationale
Massive transfusion protocol (MTP) is a tool used by clinicians when there is a need to rapidly administer a large amount of blood products, including packed red blood cells (pRBCs), fresh frozen plasma (FFP), and platelets. Complications of MTP are commonly referred to as “The Lethal Triad” referring to hypothermia, acidosis and coagulopathy.
Authors: Kayleigh Yang Arzina Jaffer
Reviewers: Jasleen Brar,
Luiza Radu, Karl Darcus*
* MD at time of publication
Intervention
Indications Initial Response Pathophysiology Transfusion Targets
≥ 3 pRBCs unit transfusion requirement in 1 hour
Shock index (heart rate/systolic blood pressure) > 1
Blood volume loss >50% in ≤3 hours
ABC Score ≥ 3 of: 1. Penetrating mechanism of injury 2. Systolic blood pressure < 90 mmHg 3. Heart rate > 120 beats per minute 4. Evidence of hemoperitoneum or hemopericardium on ultrasound (positive FAST U/S exam)
RABT Score ≥ 2 of: 1. Penetrating mechanism of injury 2. Shock index > 1 3. Positive FAST U/S 4. Known or suspected pelvic fracture
Call for help
Activate institution's MTP protocol
Send for STAT type and screen
Establish large-bore intravenous access
Fluid resuscitation
Collect and send STAT bloodwork including hemoglobin, platelet, INR, fibrinogen, electrolytes, creatinine and arterial blood gas (ABG).
Citrate present in blood products to avoid clotting during storage
Stored pRBCs break down and release potassium due to time mediated degeneration
Temporary accumulation of citrate in patient's blood with rapid use of blood products
Citrate chelates calcium
Less negative cell membrane resting potential
Anaerobic metabolism
Promotes hypocalcaemia
Changes in membrane excitability
Lactic acid buildup
Coagulopathy
(see coagulation cascade slide)
Cardiac dysrhythmias (peaked T-waves, atrial block, “sine wave”, asystolic EKG changes)
Metabolic acidosis
End organ damage
Continued blood loss
Volume overload
Avoid hypocalcemia
Avoid hyperkalemia
pH 7.35-7.45
Bleeding source control
Hemoglobin >70-90
Platelets >50 INR <1.5 Fibrinogen >1.5
Avoid dilutional coagulopathy (clotting factor dilution)
Mean Arterial Pressure (MAP) >60mmHg
Temperature >35.0°C
Slow (over 5-10 minutes) IV calcium administration
Inhaled beta agonists
Insulin/Dextrose
EKG monitoring
Sodium bicarbonate
Increase minute ventilation
Fastest control method to prevent further blood loss (i.e., packing wounds)
Early tranexamic acid administration
Administer pRBCs, FFP, and platelets in a 1:1:1 ratio (fibrinogen replacement indicated if <1.5 despite FFP)
Minimize crystalloid use
Administer crystalloids in a 3:1 ratio to estimated blood loss until blood products available
Administer vasopressors to meet target, do not overshoot
Temperature monitoring Fluid warming
↑ [Potassium] in pRBCs solution
Administration of pRBCs ↑ potassium in patient's blood
Blood loss
↓ Hemoglobin
Tissue hypoperfusion
Tissue hypoxia
↑ Diluent volume
↓ Concentration of clotting factors
Tissue death
↓ Coagulation ability
↑ Transfusion requirements
Early fluid resuscitation
Rapid transfusion of cooled or room-temperature blood products/fluids
↑ Blood pressure
Development of hypothermia
↑ Bleeding and clot dislodgement potential
↓ Enzyme activity in the coagulation cascade
↓ Coagulation ability
Legend:
Pathophysiology
Mechanism
Targets
Intervention
Published Sept 5, 2024 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2024/09/Massive-Transfusion-Protocol.jpg "Massive Transfusion Protocol: Considerations and rationale
Massive transfusion protocol (MTP) is a tool used by clinicians when there is a need to rapidly administer a large amount of blood products, including packed red blood cells (pRBCs), fresh frozen plasma (FFP), and platelets. Complications of MTP are commonly referred to as “The Lethal Triad” referring to hypothermia, acidosis and coagulopathy.
Authors: Kayleigh Yang Arzina Jaffer
Reviewers: Jasleen Brar,
Luiza Radu, Karl Darcus*
* MD at time of publication
Intervention
Indications Initial Response Pathophysiology Transfusion Targets
≥ 3 pRBCs unit transfusion requirement in 1 hour
Shock index (heart rate/systolic blood pressure) > 1
Blood volume loss >50% in ≤3 hours
ABC Score ≥ 3 of: 1. Penetrating mechanism of injury 2. Systolic blood pressure < 90 mmHg 3. Heart rate > 120 beats per minute 4. Evidence of hemoperitoneum or hemopericardium on ultrasound (positive FAST U/S exam)
RABT Score ≥ 2 of: 1. Penetrating mechanism of injury 2. Shock index > 1 3. Positive FAST U/S 4. Known or suspected pelvic fracture
Call for help
Activate institution's MTP protocol
Send for STAT type and screen
Establish large-bore intravenous access
Fluid resuscitation
Collect and send STAT bloodwork including hemoglobin, platelet, INR, fibrinogen, electrolytes, creatinine and arterial blood gas (ABG).
Citrate present in blood products to avoid clotting during storage
Stored pRBCs break down and release potassium due to time mediated degeneration
Temporary accumulation of citrate in patient's blood with rapid use of blood products
Citrate chelates calcium
Less negative cell membrane resting potential
Anaerobic metabolism
Promotes hypocalcaemia
Changes in membrane excitability
Lactic acid buildup
Coagulopathy
(see coagulation cascade slide)
Cardiac dysrhythmias (peaked T-waves, atrial block, “sine wave”, asystolic EKG changes)
Metabolic acidosis
End organ damage
Continued blood loss
Volume overload
Avoid hypocalcemia
Avoid hyperkalemia
pH 7.35-7.45
Bleeding source control
Hemoglobin >70-90
Platelets >50 INR <1.5 Fibrinogen >1.5
Avoid dilutional coagulopathy (clotting factor dilution)
Mean Arterial Pressure (MAP) >60mmHg
Temperature >35.0°C
Slow (over 5-10 minutes) IV calcium administration
Inhaled beta agonists
Insulin/Dextrose
EKG monitoring
Sodium bicarbonate
Increase minute ventilation
Fastest control method to prevent further blood loss (i.e., packing wounds)
Early tranexamic acid administration
Administer pRBCs, FFP, and platelets in a 1:1:1 ratio (fibrinogen replacement indicated if <1.5 despite FFP)
Minimize crystalloid use
Administer crystalloids in a 3:1 ratio to estimated blood loss until blood products available
Administer vasopressors to meet target, do not overshoot
Temperature monitoring Fluid warming
↑ [Potassium] in pRBCs solution
Administration of pRBCs ↑ potassium in patient's blood
Blood loss
↓ Hemoglobin
Tissue hypoperfusion
Tissue hypoxia
↑ Diluent volume
↓ Concentration of clotting factors
Tissue death
↓ Coagulation ability
↑ Transfusion requirements
Early fluid resuscitation
Rapid transfusion of cooled or room-temperature blood products/fluids
↑ Blood pressure
Development of hypothermia
↑ Bleeding and clot dislodgement potential
↓ Enzyme activity in the coagulation cascade
↓ Coagulation ability
Legend:
Pathophysiology
Mechanism
Targets
Intervention
Published Sept 5, 2024 on www.thecalgaryguide.com")
Diffuse Axonal Injury

Increased intracellular sodium creates increased osmotic pressure between extracellular and intracellular space
Water moves passively along osmotic gradient into intracellular space
Neuron swelling
Hemorrhagic lesion on MRI
calcium exchangers
Activation of voltage gated calcium channels
Calcium enters the damaged neuron
Proteolytic activity increases with elevated intracellular calcium
Activated proteases cause delayed cytoskeleton damage Damage to neuron cytoskeleton impairs transport of axonal proteins Protein accumulates within axon creating bulb structure at the terminal Disconnection of axon terminal from adjacent dendrites and cell bodies
Diffuse Axonal Injury
Axonal bulbs on pathology
Damage to cortical, subcortical, and brainstem white matter tracts leads to a constellation of symptoms
Post-traumatic seizures Damage to temporal lobe Damage to primary motor cortex Lesions in ascending reticular activating system impact consciousness
Memory deficits Motor deficits
Coma & brain death
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sep 18, 2024 on www.thecalgaryguide.com")
Malignant Hyperthermia
 & volatile anesthetic (e.g., sevoflurane, desflurane, isoflurane, halothane, NOT nitrous oxide)
Autosomal dominant mutation in ryanodine receptor (RyR1; RyR1 transports calcium out of the sarcoplasmic reticulum during muscle depolarization)
LowerthresholdforactivationofRyR1 state
Prolonged opening of RyR1
↑ Ca2+ in myocyte cytoplasm
Capacity of the reuptake protein to carry Ca2+ is overwhelmed
Sustained muscle contraction à hypermetabolic state
Malignant Hyperthermia
Vigorous exercise & heat (rare)
Rare life-threatening clinical syndrome that occurs in genetically susceptible patients upon exposure to a triggering agent
Skeletal muscle rigidity (i.e., masseter muscle spasm)
Sustained muscle contraction
Myocytes (muscle cells) deplete available ATP
Hypermetabolic state
↑ O2 consumption
↑ Heart rate to meet O2 demand
↑ CO2 production
Unexplained ↑ end tidal CO2 (early sign)
↑ Temperature
Hyperthermia (late sign)
↓ O2 supply
↑ Anaerobic metabolism
↑ Lactic acid production
Metabolic acidosis
Cell death
Leakage of muscle contents into circulation
↑ Serum creatinine kinase
Development of rhabdomyolysis (rapid breakdown of muscle tissue)
Myoglobinuria (presence of excess myoglobin in urine)
Acute kidney injury**
Hyperkalemia
Electrolyte imbalances (i.e., hyperkalemia)
Abnormal myocyte contraction
Cardiac dysfunction Dysrhythmias Cardiovascular collapse
Release of thromboplastin (converts prothrombinàthrombin) & other prothrombotic substances (promotes clot formation)
Imbalance between thrombotic & antithrombotic pathway
↑ Clot formation from activation of the extrinsic & common pathways
Disseminated intravascular coagulation**
Tachypnea (in absence of prominent mechanical ventilation)
Tachycardia (early sign)
Cardiovascular collapse
Vital organ failure Coma
**See corresponding Calgary Guide slide(s)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 25, 2015; updated Oct 2, 2024 on www.thecalgaryguide.com")
Secondary hypoglycemia Insulin Mediated

Non-insulinoma pancreatic islet cell disorder
(e.g. Non-insulinoma pancreatogenous hypoglycemia syndrome)
Nesidioblastosis (pancreatic islet tissues formed from pancreatic duct budding) formation
↑ In number & size of abnormal pancreatic beta islet cells throughout the entire pancreas
↑ Insulin production & secretion by abnormal pancreatic islet cells
↑ Glycogen synthesis
Insulin autoimmune syndrome
Autoantibodies bind to insulin molecules released post-meal
Insulin molecules unable to exert effects
Hyperglycemia Promotes insulin release
↓ Plasma glucose concentration
↓ Insulin release & ↓ total insulin levels
Insulin molecules dissociate from autoantibodies
↑ Free insulin levels (inappropriate for the ↓ plasma glucose levels)
↓ Glycogenolysis (glycogen breakdown to glucose)
Hypoglycemia
(serum glucose of <3mmol/L)
Intake of insulin secretagogues (e.g. Sulphonylureas, Meglitinide analogues)
Binds to adenosine triphosphate (ATP) dependant potassium channels on pancreatic islet cells
Inhibit potassium ion efflux through ATP-dependent potassium channels
Pancreatic islet cell depolarization
Opens voltage-gated calcium channel
Calcium influx into pancreatic islet cells
↑ Insulin release
↓ Gluconeogenesis (glucose synthesis from non-carbohydrate compounds)
Exogenous insulin intake
Suppress endogenous insulin production (by beta cells)
Low C-peptide levels
(byproduct of endogenous pro- insulin being converted to insulin)
90% caused by somatic mutations of pancreatic beta islet cells
10% due to genetic changes linked to MEN1(Multipl e endocrine neoplasia type-1) gene mutation
↑ Pancreatic islet cells proliferation
↑ Insulin secretion by hyperplastic (increasing in number) pancreatic islet cells
Neuroglycopenic symptoms (altered mental status, seizures)
Neurogenic symptoms (palpitations, tremulousness, diaphoresis
Authors: Iffat Naeem Run Xuan (Karen) Zeng Reviewers: Gurreet Bhandal Luiza Radu Yan Yu* Samuel Fineblit* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Sept 29, 2024 on www.thecalgaryguide.com")
Bone Remodeling Physiology
 activity, ↑ osteoclast (bone cells that break down bone) activity
Hyperparathyroidism ↓ Blood Ca2+
↑ Parathyroid hormone (serum Ca2+ concentration increasing hormone)
Trauma
Osteoblasts detect breach in matrix integrity
Hyperthyroidism
↑ Triiodothyronine (T3)
↑ Bone turnover
Puberty
↑ Growth hormone
↑ Blood calcium (Ca2+)
↑ Calcitonin
(reduces serum Ca2+ by ↓ renal Ca2+ reabsorption & ↑ osteoclast activity)
Net bone resorption process (bone tissue released from bones)
Surveillance osteoblasts produce receptor activator of nuclear activator kappa beta (RANKL; osteoclast stimulating protein)
Monocytes fuse into osteoclasts (cells for bone breakdown)
Osteoclast actions
Secrete HCl to dissolve hydroxyapatite (bone matrix forming inorganic mineral)
Serum markers of bone resorption: C-Telopeptide (CTX) P-Telopeptide (PTX)
Net bone formation process
Hormones activate osteoblast
Osteoblast actions
Secrete osteoprotegerin that binds RANKL
Secrete osteoid seam (a new layer of unmineralized organic bone matrix)
Osteoblasts deposit hydroxyapatite on seam
Phagocytose osteocytes within bone matrix
Authors: Andrew Wu, Jason Kreutz Reviewers:Mizuki Lopez,
Gurreet Bhandal, Luiza Radu *Samuel Fineblit
* MD at time of publication
Secrete collagenase enzyme to help digest collagen
↓ Osteoclast activity
Osteoblasts become osteocytes (mature cells) within bone
Serum markers of bone formation:
↑ Alkaline phosphatase (ALP)
↑ Bone-specific alkaline phosphatase (BSAP; an enzyme produced by osteoblasts during mineralization of bone)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Oct 4, 2024 on www.thecalgaryguide.com")
Calcium Channel Blockers
![Calcium Channel Blockers: Mechanisms & side effects
Authors:
Caroline Kokorudz Reviewers:
Rafael Sanguinetti Andrew Wu
Luiza Radu
Timothy Pollak*
* MD at time of publication
Calcium channel blocker medications
inhibit Ca2+ channels in smooth muscle
Reduction of Ca2+ influx into smooth muscle cells
Inhibits calcium-dependent aldosterone synthesis reducing Na+ & H2O resorption in renal distal tubules
Negative feedback to pituitary gland causing ↑ ACTH (adrenocorticotropic hormone)
↑ Androgens (testosterone)
Testosterone acts on gingival cells (multiple cell types that support teeth) & connective tissue matrix
Gingival hyperplasia (gum overgrowth)
Non-dihydropyridines:
(Phenylalkylamines [verapamil], Benzothiazepines [diltiazem]) less potent vasodilators & selective for heart muscle
Prevents smooth muscle contraction
Dihydropyridines:
(amlodipine, felodipine, nifedipine) vasodilate vascular smooth muscle
↓ Arterial resistance and blood pressure in coronary & peripheral arteries
Coronary artery vasodilation
↓ Pressure in coronary arteries
↑ Blood flow through coronary arteries
Reduced
ischemia relieves angina
Inhibits L-type Ca2+ channels, preventing rapid nodal depolarization
Reduces excitation of sinoatrial (SA) & atrioventricular (AV) nodal tissues
↓ Conduction speed of electrical impulses
↓ Contractile strength of cardiomyocytes (heart muscle cell)
↓ Systemic vascular resistance & cardiac
afterload (heart pumping resistance)
↑ Blood volume flowing into significantly smaller vessels
↑ Capillary blood pressure
↑ Circulation to face
Flushes (red & warm)
↓ Cardiac output
↓ Tissue perfusion & attempt to ↑ cardiac output
Worsens heart failure
↓ Oxygen demand of heart muscle
More favorable oxygen supply to demand ratio
Relieves angina
↓ Blood pressure
↓ Cerebral perfusion
Syncope (fainting)
Relieves angina
Capillary fluid leak increased to interstitial space
Peripheral edema
↑ Intracranial pressure Compresses nerve endings Headache
↓ Heart rate Bradycardia
Suppresses dysrhythmias (abnormal heart rhythm)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 21, 2024 on www.thecalgaryguide.com](https://calgaryguide.ucalgary.ca/wp-content/uploads/2024/11/Calcium-Channel-Blockers.jpg "Calcium Channel Blockers: Mechanisms & side effects
Authors:
Caroline Kokorudz Reviewers:
Rafael Sanguinetti Andrew Wu
Luiza Radu
Timothy Pollak*
* MD at time of publication
Calcium channel blocker medications
inhibit Ca2+ channels in smooth muscle
Reduction of Ca2+ influx into smooth muscle cells
Inhibits calcium-dependent aldosterone synthesis reducing Na+ & H2O resorption in renal distal tubules
Negative feedback to pituitary gland causing ↑ ACTH (adrenocorticotropic hormone)
↑ Androgens (testosterone)
Testosterone acts on gingival cells (multiple cell types that support teeth) & connective tissue matrix
Gingival hyperplasia (gum overgrowth)
Non-dihydropyridines:
(Phenylalkylamines [verapamil], Benzothiazepines [diltiazem]) less potent vasodilators & selective for heart muscle
Prevents smooth muscle contraction
Dihydropyridines:
(amlodipine, felodipine, nifedipine) vasodilate vascular smooth muscle
↓ Arterial resistance and blood pressure in coronary & peripheral arteries
Coronary artery vasodilation
↓ Pressure in coronary arteries
↑ Blood flow through coronary arteries
Reduced
ischemia relieves angina
Inhibits L-type Ca2+ channels, preventing rapid nodal depolarization
Reduces excitation of sinoatrial (SA) & atrioventricular (AV) nodal tissues
↓ Conduction speed of electrical impulses
↓ Contractile strength of cardiomyocytes (heart muscle cell)
↓ Systemic vascular resistance & cardiac
afterload (heart pumping resistance)
↑ Blood volume flowing into significantly smaller vessels
↑ Capillary blood pressure
↑ Circulation to face
Flushes (red & warm)
↓ Cardiac output
↓ Tissue perfusion & attempt to ↑ cardiac output
Worsens heart failure
↓ Oxygen demand of heart muscle
More favorable oxygen supply to demand ratio
Relieves angina
↓ Blood pressure
↓ Cerebral perfusion
Syncope (fainting)
Relieves angina
Capillary fluid leak increased to interstitial space
Peripheral edema
↑ Intracranial pressure Compresses nerve endings Headache
↓ Heart rate Bradycardia
Suppresses dysrhythmias (abnormal heart rhythm)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 21, 2024 on www.thecalgaryguide.com")
Hypocalcemia Pathogenesis

Autoimmune (e.g., autoimmune polyglandular syndrome)
Infiltrative (e.g., hemochro matosis, Wilson’s disease)
Congenital (e.g., DiGeorge)
Hypomagnesemia
Magnesium is needed to produce PTH
Malabsorption
↓ Small bowel surface area
↓ Absorption of 25-OH Vitamin D (calcidiol)
↓ Conversion of calcidiol to 1-25 (OH)2 Vitamin D (calcitriol) by 1-α- hydroxylase
↓ Calcitriol
(impacts GI absorption of calcium)
Chronic Renal Failure
↓ Renal parenchymal mass (site of 1-α- hydroxylase production)
Vitamin D Dependent Type 1 Rickets
Mutation in the gene that encodes 1-α- hydroxylase
↓ Sun exposure
↓ 1-α-hydroxylase Pancreatitis
Destruction or atrophy of parathyroid gland
↓ Parathyroid hormone (PTH)
Calcitriol resistance (e.g., Vitamin D Type 2 rickets)
Inflammation of pancreas
↑ Release of lipase enzyme into serum
↑ Breakdown of fat by lipase
↑ Free fatty acids in serum
↑ Ca2+ binding to negatively charged tail of free fatty acids
↑ Parathyroid hormone (PTH)
PTH resistance
Genetic mutation causes body to not respond to PTH
↓ Renal calcium reabsorption
↑ Calcium excretion
↓ Osteoclast activity
↓ Calcium release from bone
↓ Action of PTH on intestinal cells
↓ Absorption of calcium in the small intestine
↑ Serum phosphate (PO4) (e.g. tumor lysis, rhabdomyolysis)
↑ Ca2+
binding to
negatively charged PO4
↑ Serum pH
↓ H+ in serum binding to proteins
↑ Ca2+ binding to proteins
Calcium sequestration
↓ Absorption of calcium in the small intestine
Hypocalcemia
Author: Breanna Fang Reviewers: Gurreet Bhandal, Raafi Ali, Luiza Radu Samuel Fineblit* * MD at time of publication
Serum calcium levels below 2.10mmol/L
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Nov 22, 2024 on www.thecalgaryguide.com")
Dopamine Antagonists Metoclopramide & Domperidone
 Zeng Luiza Radu Esther Ho* * MD at time of publication
Binds to & blocks dopamine D2 receptors in the chemoreceptor trigger zone (CTZ) in medulla oblongata
Binds to & blocks
serotonin (5-HT3) receptors in the CTZ in medulla oblongata
Binds to & blocks dopamine D1 & D2 receptors in the nucleus accumbens of the basal forebrain
Binds to & blocks dopamine D2 receptors in the substantia nigra of the basal ganglia
Binds to & blocks dopamine D2 receptors in the anterior pituitary
Binds to & blocks dopamine D2 receptors in myenteric plexuses of the proximal gut
Binds to & blocks dopamine D2 receptors in the myocardium
Incoming vagal afferents (sensory nerve signals) reduce dopamine release at the CTZ
Incoming vagal afferents (sensory nerve signals) reduce serotonin release at the CTZ
↓ Binding of dopamine released by neurons in the ventral tegmental area (VTA) of the midbrain
↓ Dopamine’s inhibitory effect on neurons in the ventrolateral (VL) nucleus of the thalamus
↓ Binding of dopamine released by neurons in the hypothalamus
↑ Acetylcholine (Ach) release from parasympathetic neuronal nerve endings
↓ Dopamine binding at the CTZ
↓ Serotonin binding at CTZ
↓ Activation of wake-promoting VTA neurons
↑ Excitatory activity of neurons in the VL nucleus of the thalamus
↓ Dopamine’s inhibitory effect on prolactin secretion
Influx of calcium ions into smooth muscle
↓ Dorsal motor nucleus activity of the vagus nerve in the medulla oblongata
↓ Nucleus solitary tract activity (processes sensory signals from body)
↓ Vomiting center activity
Suppressed vomiting reflex
↓ Vomiting
Central Actions
↓ Excitatory signals to promote wakefulness
Drowsiness
Extrapyramidal symptoms (EPS; impaired motor control)
Dystonia (sustained muscle spasm & abnormal posture), akathisia (restlessness), chorea (rapid, irregular movement), parkinsonism (tremors, rigidity) EPS symptoms occur mostly with metoclopramide. Domperidone does not readily cross CNS and is less likely to produce EPS symptoms.
Continuous activation signal to corticospinal motor control system
Hyperprolactinemia
(↑ prolactin secretion)
↑ Involuntary movements
Peripheral Actions
Torsade de Pointes (polymorphic ventricular
tachycardia; rapid & irregular heart rhythm on ECG)
Membrane depolarization
↑ Velocity of excitatory waves on smooth muscle walls
↑ Gut tone & rhythm of contraction
↑ Gastric and small intestinal motility & ↑ lower esophageal sphincter tone
Blocks potassium channel
Inhibits potassium ion outflow
Delayed ventricular repolarization (>440 milliseconds in men
& >460 milliseconds in women)
Myocardium unable to compensate for arrhythmia
Ventricular fibrillation Cardiac Arrest Death
Bradycardia (Slow than normal heart rate)
Long QT Syndrome Extended QT interval seen on electrocardiogram (ECG)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Jan 28, 2025 on www.thecalgaryguide.com")
Osgood Schlatter Disease

Patellar tendon inserts more proximally or broadly on tibia
↓ Patellar tendon moment arm length causes ↑ biomechanical forces on tibial tubercle
Patella alta (superior displacement of the patella within the trochlear groove) *temporal relationship uncertain
Quadriceps require ↑ forces to achieve full extension
Patellar tendon overuse
↑ Patellar tendon tension
↑ Traction stress on the patellar tendon insertion at the cartilaginous tibial tubercle apophysis in one or both knees
Osgood-Schlatter Disease
Self-limiting osteochondrosis or traction apophysitis (inflammation of the growth plate) of the proximal tibial tubercle at the insertion of the patellar tendon
Tibial tubercle apophysis hypertrophies & develops chronic micro-avulsions (tibial apophyseal ossification centers & cartilage is pulled off the tibial metaphysis)
↑ Inflammation at injury site Proximal patellar tendon micro- Repetitive strain/forces on the proximal tibial apophysis
Tibial apophysis undergoes partial arrest
Asymmetric proximal tibial epiphyseal growth abnormality (posterior > anterior)
Genu recurvatum (knee hyperextension) (rare)
due to traction apophysitis avulses from the tibial apophysis
overcomes bone-tendon attachment strength
Activated immune cells release cytokines at injury site
Sensitization of nociceptors in periosteum and surrounding tissues
Tenderness and Antalgic swelling of gait
patellar tendon
Proximal tibial apophyseal fragmentation (visible on X-ray)
Avulsion fracture of tibial tubercle
Calcium is abnormally deposited in the tendon
Calcific tendinopathy in patellar tendon (visible on X-ray)
Anterior knee pain that worsens with exercise
Inflammatory mediators recruit osteoblast precursors to stabilize injury site
↑ Osteoblast activity drives bone remodeling and formation of ossicles (small pieces of bone)
Bone remodeling causes united ossicles (ossicle fusion with tibial tuberosity)
Ununited ossicle imbedded within patellar tendon (visible on X-ray)
Bony prominence of tibial tubercle (visible on X-ray)
Residual ununited ossicle remains after apophysis fuses with proximal tibial metaphysis
Persistent visible prominence after proximal tibial apophyseal closure
Authors: Emily J. Doucette Reviewers: Michelle J. Chan Yan Yu* Gerhard Kiefer* * MD at time of publication
Persistent pain & discomfort with ↓ strength & function
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Feb 16, 2025 on www.thecalgaryguide.com")